Your new post is loading...
Your new post is loading...
Attitudes to paediatric COVID-19 vaccination from Taiwan 🇹🇼
Traditional media is still a common source of information, thankfully, but with strong evidence…
Read the original article in full on F1000Research: Sentiment analysis of Indonesian tweets on COVID-19 and COVID-19 vaccinations...
The debate around vaccines has been going on for decades, but the COVID-19 pandemic showed how crucial it is to understand and mitigate anti-vaccine sentiments. While the pandemic may be over, it is still important to understand how the pandemic affected the anti-vaccine discourse, and whether the...
Authors Thamyres Maria Silva Barbosa Stefany Medeiros Castello Branco Amanda Soares do Amaral Lucas Ramos Maran Eriselma Alves Correia Adriana Siqueira de Sá Alexandre Maslinkiewicz Geoeselita Borges Teixeira João Pedro Neto de Sousa DOI: https://doi.org/10.55905/revconv.17n.2-136 Keywords:...
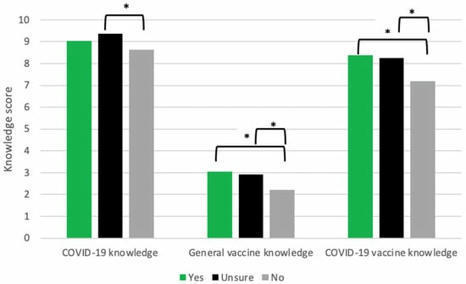
The current study examined various types of misinformation related to the COVID-19 vaccines and their relationships to vaccine hesitancy and refusal. Study 1 asked a sample of full-time working professionals in the US (n = 505) about possible misinformation they were exposed to related to the COVID-19 vaccines. Study 2 utilized an online survey to examine U.S. college students’ (n = 441) knowledge about COVID-19 vaccines, and its associations with vaccine hesitancy and behavioral intention to get a COVID-19 vaccine. Analysis of open-ended responses in Study 1 revealed that 57.6% reported being exposed to conspiratorial misinformation such as COVID-19 vaccines are harmful and dangerous. The results of a structural equation modeling analysis for Study 2 supported our hypotheses predicting a negative association between the knowledge level and vaccine hesitancy and between vaccine hesitancy and behavioral intention. Vaccine hesitancy mediated the relationship between the vaccine knowledge and behavioral intention. Findings across these studies suggest exposure to misinformation and believing it as true could increase vaccine hesitancy and reduce behavioral intention to get vaccinated.
Avant la pandémie de Covid-19, l’Organisation mondiale de la santé (OMS) avait placé le refus vaccinal au rang de l’une des trois plus grandes urgences de santé publique mondiale. L’OMS a constaté une chute régulière de la couverture vaccinale contre la rougeole et une recrudescence des épidémies dans le monde. Dans le même temps, les sites Internet antivaccin ont proliféré et ont fait de nombreux adeptes en usant de désinformation et de théories du complot. Ces « antivaccin », du parent a
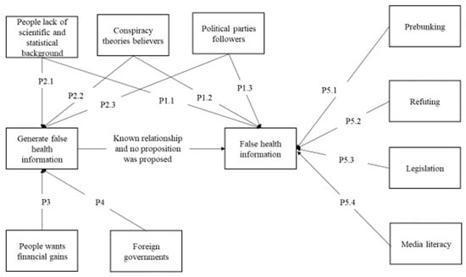
The COVID-19 pandemic heightened concerns about health and safety, leading people to seek information to protect themselves from infection. Even before the pandemic, false health information was spreading on social media.
Kai Ruggeri, professor1, Samantha Vanderslott, associate professor2, Yuki Yamada, associate professor3, Young Anna Argyris, associate professor4, Bojana Većkalov, doctoral student5, Paulo Sergio Boggio, director6, Mosoka P Fallah, programme manager7, Friederike Stock, doctoral student8, Ralph Hertwig, professor91Department of Health Policy and Management, Mailman School of Public Health, Columbia University, New York City, NY, USA2Vaccines and Society Unit, Oxford Vaccine Group, Centre for Clinical Vaccinology and Tropical Medicine, Churchill Hospital, NIHR Oxford Biomedical Research Centre, Oxford, UK3Faculty of Arts and Science, Kyushu University, Fukuoka, Japan4Department of Media and Information, Michigan State University, East Lansing, MI, USA5Department of Psychology, University of Amsterdam, Amsterdam, Netherlands6Cognitive and Social Neuroscience Laboratory, Mackenzie Presbyterian University, São Paulo, Brazil7Saving Lives and Livelihoods, Africa Center for Disease Control, Addis Ababa, Ethiopia8Center for Adaptive Rationality, Max Planck Institute for Human Development, Berlin, Germany9Max Planck Institute for Human Development, Berlin, GermanyCorrespondence to: K Ruggeri kai.ruggeri{at}columbia.eduKey messagesSubstantial evidence shows the negative effects of vaccine misinformation on social mediaEvidence on the effectiveness of interventions to correct or mitigate misinformation is considerably more limited and rarely includes measures of true vaccine uptakeThe evidence available does indicate ways forward to develop better methods, particularly those that would be less likely to backfire in the way that blanket social media bans haveThe need for such actions is urgentVaccine misinformation on social media has strong effects on behaviour, and the evidence base for interventions to reduce these effects is limited, but better approaches to evidence generation are possible, say Kai Ruggeri and colleaguesEffective population level vaccination campaigns are fundamental to public health.123 Counter campaigns, which are as old as the first vaccines,4 disrupt uptake and can threaten public health globally.4 In 2019, public health researchers linked increases in measles cases with the proliferation of global anti-vaccine campaigns.5 Some of these campaigns originated offline but were later amplified and expedited through social media, resulting in real world harms.6 Though crises and genuine safety concerns can also lower vaccine uptake,78 the return of measles after aggressive anti-vaccine campaigns prompted the World Health Organisation to list vaccine hesitancy among the greatest threats to global health (box 1).14Box 1 Vaccine hesitancyHere, we use the term “vaccine hesitancy” as originally defined by WHO9: a “delay in acceptance or refusal of vaccination despite availability of vaccination services.” This definition, plus the expanded description of variation based on time, place, and population, gives a broad understanding but also allows us to distinguish vaccination behaviour from the underpinning psychological, environmental, and structural aspects influencing behaviour. This definition is most commonly used in literature pre-dating covid-19. Though there are debates about the most appropriate terms (“vaccine demand” is an alternative, for example) or updated definitions (including the updated WHO version) to use, applying the original WHO definition ensured that we captured relevant insights and evidence from the literature.10111213 We also identify disinformation as a form of misinformation that deliberately seeks to mislead or otherwise disrupt understanding, although we cover both broadly under misinformation for the purposes of this paper.RETURN TO TEXTAnti-vaccine campaigns proliferated during the covid-19 pandemic15 with undeniable effects including substantial increases in covid related illness and death.151617 Even before March 2020, vaccine hesitancy was directly linked to misinformation (false, inaccurate information promoted as factual) spread on social media.18 Once covid-19 reached pandemic status, social media was acknowledged as the epicentre of misinformation leading to hesitancy,1920 and consequently, interventions to tackle hesitancy have globally focused on delivery through social media.2122Despite unprecedented levels of vaccine access and nearly real time communication on the development and availability of vaccines in 2020-21, public health officials struggled to keep pace with misleading or inaccurate content online.23 As guidelines shifted with the emergence of new information, policy decisions were often perceived by individuals and groups who are prone to distrust or refute government messaging as a response not to evidence but to mistakes or lack of expertise.2425 A 2021 randomised controlled trial (RCT) found that exposure to misinformation about covid-19 vaccines lowered the intent of recipients to vaccinate, even among those reporting before exposure that they would “definitely” accept vaccination.21 Similar findings globally indicate that social media dynamics exacerbated the sharing of misinformation, reduced vaccination rates, undermined trust in reliable information, magnified polarisation, and damaged the perceived credibility of institutions.2627282930 These challenges remain today.Approaches to reducing vaccine hesitancyStandard behavioural approaches to encourage vaccination include mandatory vaccination and regulation for healthcare professionals, incentives, public health communication campaigns, and engaging trusted leaders.31 Contemporary methods have started to be implemented on social media,10313233 including debunking (fact checking specific claims after they have reached social media users) and “pre-bunking,” a behavioural approach in which users are taught about how “fake news” works before exposure.34 Other intervention types include warning (“inoculating”) people about manipulation tactics using non-harmful exposure as a tool to identify misinformation, and using accuracy prompts to trigger people to consider the truthfulness of material they are about to share on social media platforms, without stopping them from posting.35 Recognising the intense effect of social media on vaccine hesitancy,36 the Africa Centres for Disease Control and Prevention developed a toolkit to assist countries in social media strategies aimed at encouraging vaccination.37Such behavioural approaches to misinformation on social media have shown promise in reducing the sharing of disinformation and misinformation (box 1) and in changing people’s beliefs,38 but less clear is their effect on vaccination uptake. Investigating the success of such interventions on uptake is essential because there is an established link between social media exposure and offline beliefs that vaccines are unsafe.39 It is clear, however, that providing fact based probabilistic information alone fails to meaningfully increase uptake40 and might even backfire.41 Factors such as low trust in governments and health institutions are likely to be instrumental in derailing effective immunisation programmmes.42 Multiple drivers and barriers to vaccine uptake must therefore be considered when developing effective tools.Evaluating interventions to reduce vaccine hesitancyWe identified 30 studies evaluating interventions to tackle misinformation on social media that explicitly captured real world behavioural outcomes (see supplementary information on bmj.com). After excluding 19 studies for lack of external validation, only 11 published interventions were left (table 1; box 2; fig 1). There is clearly insufficient evidence from field studies on social media interventions. Only two interventions that met all criteria came from outside the US (Israel43 and Nigeria53), with a recent study conducted in Nigeria producing perhaps the most robust level of evidence.Table 1 Interventions to reduce vaccine hesitancy through social media that assessed real world vaccine behavioursView popupView inlineBox 2 A robust research agenda for social media interventions is neededStudies on reducing vaccine hesitancy can inform broader vaccination messaging campaigns. We recommend some critical features that should be included for all interventions (fig 1). Details about the type of vaccine and the target group should be highly specific, as should the form of hesitancy and misinformation,54 the misinformation source, and details of the method (especially for RCTs). Real world effects (ideally direct and broader public health indicators) must be captured. These aspects are relevant for better understanding of what might work and for what reasons and for comparison between methods and social media platforms. The most informative approach would cover the first three levels of evidence under the THEARI system (theoretical, empirical, and real world).55 Over time, these would accumulate to the fourth (replicated) and fifth (well established impact) levels, maximising the potential for predictive validity of applications to public policy (for example, greater confidence in anticipated effects). Doing so would exceed the criteria listed in a recent call for a gold standard for trials tackling vaccine hesitancy.56RETURN TO TEXTFig 1 Critical aspects of studies that are necessary to better understand and compare possible interventions that tackle vaccine hesitancy on social media (described in box 2). The examples of what specifically to measure and observe are non-exhaustive. All aspects should be included for maximum value, though behavioural and population health outcomes should be prioritised. Boxes with thick outlines and darker shading are considered absolutely necessary, though all boxes are strongly recommended.Download figure Open in new tab Download powerpoint Some evidence exists from field studies that did not directly target misinformation but provided accurate and useful information about vaccines. These were typically posted on interactive websites or directly in social media feeds. Changes in attitudes, knowledge, and social media engagement were reported for several information campaigns using social media advertisements in before and after designs and designs without control groups.44454748 But these studies showed no changes in vaccination behaviours. Only two studies, both RCTs, showed that tackling vaccination concerns and providing information in interactive formats on a website increased vaccination46 and reduced days undervaccinated.51Two interventions that increased vaccination uptake used targeted messages through Facebook adverts57 and personalised influencer content.58 But each had limitations. In the first, vaccination rates increased only among families of medium-low socioeconomic status, indicating narrow effectiveness. In the second, the measures were primarily attitudinal, and behavioural outcomes were self-reported.Linking online campaigns to true behaviours in field studies is a major challenge. This is partly because running well controlled studies is simpler in laboratory experiments and surveys, and because capturing distal effects (true behaviours) of web based studies is often impossible. But showing some measures of success in increasing uptake is necessary to justify investment to develop interventions at scale. Therefore, it is critical that researchers of vaccine behaviours and associated campaigns engage directly with clinics and public health agencies to improve the ecological and external validity (that is, real world, observed outcomes) of interventions (box 2).Developing better interventions to confront vaccine hesitancy on social mediaFew interventions among those we evaluated captured evidence about real world behaviours, so there is currently no gold standard toolkit that public health agencies can refer to.56 But the evidence available can inform future tool development. We provide 10 insights based on the existing evidence that should help provide a clearer and more specific, evidence driven toolkit of approaches to reduce vaccine hesitancy.Negative sentiments on social media might increase vaccine hesitancy faster than interventions reduce it3959—Although vaccine hesitancy can stem from many sources, including mass media and political rhetoric as well as genuine safety concerns, there is ample evidence of a proliferation of anti-vaccine messages on social media leading to organised offline actions and increased hesitancy.60 This is driven by several social and individual factors, as well as foreign disinformation campaigns and bots.6162 There is less evidence that efforts to specifically mitigate misinformation have had a reliable effect on real world vaccine uptake.Messaging seems to work best when it is tailored to what groups know and care about—Two relatively large vaccination interventions, one for flu, one for human papillomavirus (HPV), found modest effects through targeting specific groups. Broad campaigns through all forms of media tend to be generally effective. But once misinformation and conflicting views are prevalent, speaking directly to audiences, knowing the reasons for hesitancy, and framing information in a way that matters to individuals are critical.546364Simple messaging about benefits and risk based on probabilities is not enough—Filling vaccine knowledge gaps has direct benefits, such as supporting informed decisions,63 but messaging with information about benefits, harms, and associated probabilities is insufficient to resolve vaccine hesitancy.40 Some possible explanations include lack of trust and cultural values, which have a major effect on how scientific data are interpreted and accepted through social media.65 Messages must be conveyed in a way that affirms individual cultural values,66 dealing with topics of importance to individuals, not only health facts, using credible sources of information.67 Visual imagery also helps deliver effective messages,68 and other components should be considered, such as health literacy, simplified language, and context specific features like age or language.Correct misinformation to both parents and their children—Parents, especially mothers, play a major part in child vaccination.58 One large campaign carried out on Facebook directed at mothers of teens had some positive effects in specific income groups, but the overall effect was minimal to null. Addressing parents is clearly of value, but young people also seek out information online for themselves.69 Thus, the information teens are presented with online likely needs similar but unique safeguards against misinformation to the ones discussed. Directly involving parents and young people in the design of messaging might strengthen the effectiveness of these campaigns.70Trust matters: the message,71the messenger,63and the (vaccinated) provider57—Substantial amounts of anti-vaccine messaging comes from non-medically qualified, or non-expert, voices on social media.72 Thus, medical professionals are under-represented when it comes to legitimate and accurate information about vaccines on social media,73 despite typically being the most trusted sources (especially among parents74). Trust is potentially the most distinct characteristic of successful vaccination campaigns,5075 and this includes ones delivered on social media.76 Ultimately, the source of the message—whether a healthcare provider, a politician, or a social media influencer—is likely to have a major role in whether individuals and communities deem information to be credible.5763 These interventions have great potential when delivered to the right population.30 The US state of New York, for example, was a stronghold of anti-vaccine sentiment before 2020, which pivoted after the arrival of covid-19 vaccines. Despite intensifying hesitancy and misinformation waves, the state outpaced the national average for vaccination rates, benefiting both public health77 and economic returns.78 This success is attributed to strategies that, on top of tackling misinformation, also cultivated trust in the source of the vaccine, the messenger, and the provider, involving use of the military (a highly trusted organisation in the US), diverse community messengers (including community health workers and faith leaders), and a broad network of vaccination locations.79808182 These aspects must be ensured in public campaigns aimed at specific groups, especially those who are vaccine hesitant.64Debunking efforts have shown mixed effects on social media—Distributing information from public institutions or providing objective information from third parties might help to counter misinformation, reduce the intention to spread misinformation, and promote health behaviours, but the process is not always smooth. The backfire effect is a concerning pattern in which disproving misinformation reinforces it and deepens false beliefs.83 But this phenomenon is not consistently observed in practice. Effects of debunking might be highly dependent on the recipient’s background knowledge and beliefs, methods of presentation, and what other information is viewed.8485 For now, the immediate priority for this approach is to determine if inoculation based on pre-bunking can reliably reduce the noxious effects of next widespread waves of misinformation and resulting misbeliefs.Raising the quality and visibility of reliable health information can counter misinformation—Providing simple probabilistic information is not likely to completely counteract misinformation on its own, but providing information on how, where, and when to get a vaccine does.76 The high volume of misinformation appearing in online searches, however, can override more reliable sources,86 limiting the effectiveness of high-quality information campaigns.87 To increase campaign effectiveness, interactive designs and visual aids such as posters or videos help target populations see and engage with accurate, accessible information throughout a campaign.51 Making it easier to find such materials is paramount, starting with search engine optimisation to increase visibility of campaigns.Framing of vaccine messages matters—How public campaign messaging is framed affects health decision making. A public campaign can’t cover all vaccines, diseases, populations, and reasons for hesitancy; framing messages to be directly relevant to a populations’ needs (benefits and risks specific to their group) have resulted in significant increases in uptake.88 Positive and negative framing effects are not equivalent,89 however, and this should be factored into messaging decisions.Blanket bans can drive groups and activities underground—Broad social media bans of individuals or of specific content can paradoxically result in the spread of misinformation and can galvanise problematic echo chambers by driving discussion into private social media groups or closed forums.9091 Such closed environments are unlikely to include different viewpoints or corrective information, so misinformation is more likely to be reinforced. Rather than rely on outright bans, policy makers and content managers should explore methods that limit the spread and influence of misinformation.92Social media platforms need to be part of the solution—If social media platforms are the epicentre of misinformation, then social media companies need to be part of the solution.39 During the covid-19 pandemic, social media platforms took a more interventionist approach to content moderation than before (and, in some cases, removed or limited covid-19 misinformation and conspiracies).93 Some of these approaches are now being rolled back, and social media researchers’ access to data about behaviour on the global platform X (formerly Twitter) is being limited. Content labelling and corrective actions have produced some positive effects,94 but social media companies should be more proactive in dealing with the proliferation of misinformation on their sites.95 We endorse calls39 to make data available and to work with researchers and regulators in all countries to enable developing effective solutions.It is worth it to get these campaigns rightMisinformation is not new and its noxious consequences are not insurmountable, but its effect on vaccine hesitancy through social media is an urgent global threat to public health. Increasingly robust evidence has shown the drivers and effects of this phenomenon, but few successful, let alone replicated, interventions exist. One important step towards developing more effective interventions is the close monitoring of public perceptions and opinions about vaccination and services. Digital technologies make it possible to analyse large quantities of “social listening data” in real time.96 Such information would complement the evidence we already have from a variety of study types, improving the design of new, robust, and appropriately targeted interventions. Because most published interventions focused on attitudes and intentions rather than on actual vaccination, however, there remains an urgent need for direct partnerships between behavioural researchers with healthcare clinics and public health agencies.77 Meaningfully developing those partnerships promises direct benefits for more reliable scientific insights that would improve the health and well being of entire populations.AcknowledgmentsWe thank Valentina Cafarelli for assistance with reviewing interventions identified during the search.FootnotesContributors and sources: KR conceived the idea. BV and FS were involved in the conceptualisation and delivery of the literature search, with support from YAA. KR and FS reviewed and extracted information from studies. YY, RH, SV, YAA contributed to the first draft of the manuscript. All co-authors reviewed and provided insightful comments to subsequent manuscript drafts. KR and PSB provided earlier drafts of the figure in box 2. All authors approved the final report. KR is responsible for the overall content as the guarantor of this work.Provenance and peer review: Commissioned; externally peer reviewed.Patient and public involvement: No patients or general members of the public were asked to participate given this Analysis did not relate to clinical care or health services. The focus of the article was to summarise available evidence and provide directions for future research.Competing interests: All authors confirm that they have no conflicts or competing interests in contributing to this manuscript.The article is part of a collection that was proposed by the Advancing Health Online Initiative (AHO), a consortium of partners including Meta and MSD, and several non-profit collaborators (https://www.bmj.com/social-media-influencing-vaccination). Research articles were submitted following invitations by The BMJ and associated BMJ journals, after consideration by an internal BMJ committee. Non-research articles were independently commissioned by The BMJ with advice from Sander van der Linden, Alison Buttenheim, Briony Swire-Thompson, and Charles Shey Wiysonge. Peer review, editing, and decisions to publish articles were carried out by the respective BMJ journals. Emma Veitch was the editor for this collection.http://creativecommons.org/licenses/by-nc/4.0/This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.References↵Carter A, Msemburi W, Sim SY, et al. Modeling the impact of vaccination for the immunization Agenda 2030: Deaths averted due to vaccination against 14 pathogens in 194 countries from 2021 to 2030. Vaccine2023;S0264-410X(23)00854-X. doi:10.1016/j.vaccine.2023.07.033 pmid:37537094OpenUrlCrossRefPubMed↵Centers for Disease Control and Prevention. Why CDC is involved in global immunization. 2023. https://www.cdc.gov/globalhealth/immunization/why/index.html.↵Sim SY, Watts E, Constenla D, Brenzel L, Patenaude BN. Return on investment from immunization against 10 pathogens in 94 low- and middle-income countries, 2011-30. Health Aff (Millwood)2020;39:1343-53. doi:10.1377/hlthaff.2020.00103 pmid:32744930OpenUrlCrossRefPubMed↵Mutombo PN, Fallah MP, Munodawafa D, et al. COVID-19 vaccine hesitancy in Africa: a call to action. Lancet Glob Health2022;10:e320-1. doi:10.1016/S2214-109X(21)00563-5 pmid:34942117OpenUrlCrossRefPubMed↵Hotez PJ, Nuzhath T, Colwell B. Combating vaccine hesitancy and other 21st century social determinants in the global fight against measles. Curr Opin Virol2020;41:1-7. doi:10.1016/j.coviro.2020.01.001 pmid:32113136OpenUrlCrossRefPubMed↵Dyer O. Measles outbreak in Somali American community follows anti-vaccine talks. BMJ2017;357:j2378. doi:10.1136/bmj.j2378 pmid:28512183OpenUrlFREE Full Text↵Lam E, McCarthy A, Brennan M. Vaccine-preventable diseases in humanitarian emergencies among refugee and internally-displaced populations. Hum Vaccin Immunother2015;11:2627-36. doi:10.1080/21645515.2015.1096457 pmid:26406333OpenUrlCrossRefPubMed↵Cooper S, Gadanya M, Kaawa-Mafigir D, et al. Using social media to build confidence in vaccines: lessons from community engagement and social science research in Africa. BMJ2023;383:e075564↵MacDonald NE, SAGE Working Group on Vaccine Hesitancy. Vaccine hesitancy: definition, scope and determinants. Vaccine2015;33:4161-4. doi:10.1016/j.vaccine.2015.04.036 pmid:25896383OpenUrlCrossRefPubMed↵Larson HJ, Gakidou E, Murray CJL. The vaccine-hesitant moment. N Engl J Med2022;387:58-65. doi:10.1056/NEJMra2106441 pmid:35767527OpenUrlCrossRefPubMed↵Dudley MZ, Privor-Dumm L, Dubé È, MacDonald NE. Words matter: vaccine hesitancy, vaccine demand, vaccine confidence, herd immunity and mandatory vaccination. Vaccine2020;38:709-11. doi:10.1016/j.vaccine.2019.11.056 pmid:31836257OpenUrlCrossRefPubMed↵Bussink-Voorend D, Hautvast JLA, Vandeberg L, Visser O, Hulscher MEJL. A systematic literature review to clarify the concept of vaccine hesitancy. Nat Hum Behav2022;6:1634-48. doi:10.1038/s41562-022-01431-6 pmid:35995837OpenUrlCrossRefPubMed↵World Health Organization. Understanding the behavioural and social drivers of vaccine uptake WHO position paper—May 2022. https://www.who.int/publications-detail-redirect/who-wer9720-209-224.↵Nohynek H, Arora N, Binka F, et al. Report of the Expert Advisory Group on SAGE Evaluation (EAGSE). https://cdn.who.int/media/docs/default-source/immunization/sage/sage-evaluation-2019/sage_evaluation_report_2019_print_final.pdf↵Unicef. New data indicates declining confidence in childhood vaccines of up to 44 percentage points in some countries during the covid-19 pandemic. https://www.unicef.org/press-releases/sowc_2023_immunization↵Karafillakis E, Van Damme P, Hendrickx G, Larson HJ. COVID-19 in Europe: new challenges for addressing vaccine hesitancy. Lancet2022;399:699-701. doi:10.1016/S0140-6736(22)00150-7 pmid:35123665OpenUrlCrossRefPubMed↵Council of Canadian Academies. Fault lines. The Expert Panel on the Socioeconomic Impacts of Science and Health Misinformation. 26 Jan 2023. https://cca-reports.ca/reports/the-socioeconomic-impacts-of-health-and-science-misinformation/.↵Burki T. Vaccine misinformation and social media. Lancet Digit Health2019;1:e258-9doi:10.1016/S2589-7500(19)30136-0OpenUrlCrossRef↵Razai MS, Chaudhry UAR, Doerholt K, Bauld L, Majeed A. Covid-19 vaccination hesitancy. BMJ2021;373:n1138. doi:10.1136/bmj.n1138 pmid:34016653OpenUrlFREE Full Text↵Solís Arce JS, Warren SS, Meriggi NF, et al. COVID-19 vaccine acceptance and hesitancy in low- and middle-income countries. Nat Med2021;27:1385-94. doi:10.1038/s41591-021-01454-y pmid:34272499OpenUrlCrossRefPubMed↵Loomba S, de Figueiredo A, Piatek SJ, de Graaf K, Larson HJ. Measuring the impact of COVID-19 vaccine misinformation on vaccination intent in the UK and USA. Nat Hum Behav2021;5:337-48. doi:10.1038/s41562-021-01056-1 pmid:33547453OpenUrlCrossRefPubMed↵Arechar AA, Allen J, Berinsky AJ, et al. Understanding and combatting misinformation across 16 countries on six continents. Nat Hum Behav2023;7:1502-13. doi:10.1038/s41562-023-01641-6 pmid:37386111OpenUrlCrossRefPubMed↵Ruggeri K, Stock F, Haslam SA, et al. A synthesis of evidence for policy from behavioral science during covid. Nature2023; https://doi.org/10.1038/s41586-023-06840-9↵Wegwarth O, Hertwig R, Giese H, Fineberg HV. The impact of nontransparent health communication during the covid-19 pandemic on vaccine- hesitant people’s perception of vaccines. Preprint. 2023doi:10.31219/osf.io/znwyx. ↵Stephenson-Hunter C, Yusuf Y, Larson R, Campanella J, Gutnick DN. What matters to us: bridging research and accurate information through dialogue (BRAID) to build community trust and cultivate vaccine confidence. Prev Med Rep2023;34:102253. doi:10.1016/j.pmedr.2023.102253 pmid:37252070OpenUrlCrossRefPubMed↵Pierri F, Perry BL, DeVerna MR, et al. Online misinformation is linked to early COVID-19 vaccination hesitancy and refusal. Sci Rep2022;12:5966. doi:10.1038/s41598-022-10070-w pmid:35474313OpenUrlCrossRefPubMed↵Fridman A, Gershon R, Gneezy A. COVID-19 and vaccine hesitancy: A longitudinal study. PLoS One2021;16:e0250123. doi:10.1371/journal.pone.0250123 pmid:33861765OpenUrlCrossRefPubMed↵Yang K-C, et al. The covid-19 infodemic: Twitter versus Facebook. Big Data Soc2021;8:20539517211013860doi:10.1177/20539517211013861OpenUrlCrossRef↵Wallace J, Goldsmith-Pinkham P, Schwartz JL. Excess death rates for Republican and Democratic registered voters in Florida and Ohio during the covid-19 pandemic. JAMA Intern Med2023;183:916-23. doi:10.1001/jamainternmed.2023.1154 pmid:37486680OpenUrlCrossRefPubMed↵Larsen BJ, Ryan TJ, Greene S, Hetherington MJ, Maxwell R, Tadelis S. Counter-stereotypical messaging and partisan cues: Moving the needle on vaccines in a polarized United States. Sci Adv2023;9:eadg9434. doi:10.1126/sciadv.adg9434 pmid:37467319OpenUrlCrossRefPubMed↵Cameron-Blake E, Tatlow H, Andretti B, et al. A panel dataset of covid-19 vaccination policies in 185 countries. Nat Hum Behav2023;7:1402-13. doi:10.1038/s41562-023-01615-8 pmid:37414885OpenUrlCrossRefPubMed↵Pluviano S, Watt C, Della Sala S. Misinformation lingers in memory: Failure of three pro-vaccination strategies. PLoS One2017;12:e0181640. doi:10.1371/journal.pone.0181640 pmid:28749996OpenUrlCrossRefPubMed↵Lazer DMJ, Baum MA, Benkler Y, et al. The science of fake news. Science2018;359:1094-6. doi:10.1126/science.aao2998 pmid:29590025OpenUrlAbstract/FREE Full Text↵Basol M, et al. Towards psychological herd immunity: Cross-cultural evidence for two prebunking interventions against COVID-19 misinformation. Big Data Soc2021;8:20539517211013868doi:10.1177/20539517211013868OpenUrlCrossRef↵Pennycook G, Rand DG. Accuracy prompts are a replicable and generalizable approach for reducing the spread of misinformation. Nat Commun2022;13:2333. doi:10.1038/s41467-022-30073-5 pmid:35484277OpenUrlCrossRefPubMed↵Osuagwu UL, Mashige KP, Ovenseri-Ogbomo G, et al. The impact of information sources on COVID-19 vaccine hesitancy and resistance in sub-Saharan Africa. BMC Public Health2023;23:38. doi:10.1186/s12889-022-14972-2 pmid:36609264OpenUrlCrossRefPubMed↵Africa CDC. Covid-19 social media support kit. https://africacdc.org/download/covid-19-social-media-support-kit/↵Pennycook G, Rand DG. Nudging social media toward accuracy. Ann Am Acad Pol Soc Sci2022;700:152-64. doi:10.1177/00027162221092342 pmid:35558818OpenUrlCrossRefPubMed↵Wilson SL, Wiysonge C. Social media and vaccine hesitancy. BMJ Glob Health2020;5:e004206. doi:10.1136/bmjgh-2020-004206 pmid:33097547OpenUrlAbstract/FREE Full Text↵Dubé E, Laberge C, Guay M, Bramadat P, Roy R, Bettinger J. Vaccine hesitancy: an overview. Hum Vaccin Immunother2013;9:1763-73. doi:10.4161/hv.24657 pmid:23584253OpenUrlCrossRefPubMed↵Nyhan B, Reifler J. Does correcting myths about the flu vaccine work? An experimental evaluation of the effects of corrective information. Vaccine2015;33:459-64. doi:10.1016/j.vaccine.2014.11.017 pmid:25499651OpenUrlCrossRefPubMed↵Goldenberg MJ. Vaccine hesitancy: public trust, expertise, and the war on science.University of Pittsburgh Press, 2021doi:10.2307/j.ctv1ghv4s4OpenUrlCrossRef↵Chodick G, Teper GR, Levi S, et al. The impact of a Facebook campaign among mothers on HPV vaccine uptake among their daughters: A randomized field study. Gynecol Oncol2021;160:106-11. doi:10.1016/j.ygyno.2020.10.037 pmid:33162176OpenUrlCrossRefPubMed↵Brandt HM, Sundstrom B, Monroe CM, et al. Evaluating a technology-mediated HPV vaccination awareness intervention: a controlled, quasi-experimental, mixed methods study. Vaccines (Basel)2020;8:749. doi:10.3390/vaccines8040749 pmid:33321975OpenUrlCrossRefPubMed↵Bonnevie E, Rosenberg SD, Kummeth C, Goldbarg J, Wartella E, Smyser J. Using social media influencers to increase knowledge and positive attitudes toward the flu vaccine. PLoS One2020;15:e0240828. doi:10.1371/journal.pone.0240828 pmid:33064738OpenUrlCrossRefPubMed↵O’Leary ST, Narwaney KJ, Wagner NM, Kraus CR, Omer SB, Glanz JM. Efficacy of a web-based intervention to increase uptake of maternal vaccines: An RCT. Am J Prev Med2019;57:e125-33. doi:10.1016/j.amepre.2019.05.018 pmid:31471001OpenUrlCrossRefPubMed↵Ortiz RR, Shafer A, Cates J, Coyne-Beasley T. Development and evaluation of a social media health intervention to improve adolescents’ knowledge about and vaccination against the human papillomavirus. Glob Pediatr Health2018;5:X18777918. doi:10.1177/2333794X18777918 pmid:29872667OpenUrlCrossRefPubMed↵Mohanty S, Leader AE, Gibeau E, Johnson C. Using Facebook to reach adolescents for human papillomavirus (HPV) vaccination. Vaccine2018;36:5955-61. doi:10.1016/j.vaccine.2018.08.060 pmid:30172634OpenUrlCrossRefPubMedSundstrom B, Brandt HM, Gray L, Young Pierce J. It’s my time: applying the health belief model to prevent cervical cancer among college-age women. J Commun Manag (Lond)2018;22:161-78doi:10.1108/JCOM-06-2016-0044OpenUrlCrossRef↵Huang JJ, Francesconi M, Cooper MH, Covello A, Guo M, Gharib SD. Community health workers on a college campus: Effects on influenza vaccination. J Am Coll Health2018;66:317-23. doi:10.1080/07448481.2018.1440582 pmid:29447623OpenUrlCrossRefPubMed↵Glanz JM, Wagner NM, Narwaney KJ, et al. Web-based social media intervention to increase vaccine acceptance: a randomized controlled trial. Pediatrics2017;140:e20171117. doi:10.1542/peds.2017-1117 pmid:29109107OpenUrlCrossRefPubMedShropshire AM, Brent-Hotchkiss R, Andrews UK. Mass media campaign impacts influenza vaccine obtainment of university students. J Am Coll Health2013;61:435-43. doi:10.1080/07448481.2013.830619 pmid:24152021OpenUrlCrossRefPubMed↵Evans WD, Bingenheimer JB, Long M, et al. Outcomes of a social media campaign to promote covid-19 vaccination in Nigeria. PLoS One2023;18:e0290757. doi:10.1371/journal.pone.0290757 pmid:37713381OpenUrlCrossRefPubMed↵Fasce A, Schmid P, Holford DL, Bates L, Gurevych I, Lewandowsky S. A taxonomy of anti-vaccination arguments from a systematic literature review and text modelling. Nat Hum Behav2023;7:1462-80. doi:10.1038/s41562-023-01644-3 pmid:37460761OpenUrlCrossRefPubMed↵Ruggeri K, van der Linden S, Wang YC, Papa F, Riesch J, Green J. Standards for evidence in policy decision-making. Nature Research Social and Behavioural Science. 5 Jun 2020. go.nature.com/2zdTQIs↵van der Linden S. We need a gold standard for randomised control trials studying misinformation and vaccine hesitancy on social media. BMJ2023;381:1007. doi:10.1136/bmj.p1007 pmid:37146997OpenUrlCrossRefPubMed↵Bartoš V, Bauer M, Cahlíková J, Chytilová J. Communicating doctors’ consensus persistently increases COVID-19 vaccinations. Nature2022;606:542-9. doi:10.1038/s41586-022-04805-y pmid:35650433OpenUrlCrossRefPubMed↵Argyris YA, Kim Y, Roscizewski A, Song W. The mediating role of vaccine hesitancy between maternal engagement with anti- and pro-vaccine social media posts and adolescent HPV-vaccine uptake rates in the US: The perspective of loss aversion in emotion-laden decision circumstances. Soc Sci Med2021;282:114043. doi:10.1016/j.socscimed.2021.114043 pmid:34147269OpenUrlCrossRefPubMed↵Rathje S, He JK, Roozenbeek J, Van Bavel JJ, van der Linden S. Social media behavior is associated with vaccine hesitancy. PNAS Nexus2022;1:pgac207. doi:10.1093/pnasnexus/pgac207 pmid:36714849OpenUrlCrossRefPubMed↵Martin S, Vanderslott S. “Any idea how fast ‘It’s just a mask!’ can turn into ‘It’s just a vaccine!’”: From mask mandates to vaccine mandates during the COVID-19 pandemic. Vaccine2022;40:7488-99. doi:10.1016/j.vaccine.2021.10.031 pmid:34823912OpenUrlCrossRefPubMed↵Yuan X, Schuchard RJ, Crooks AT. Examining emergent communities and social bots within the polarized online vaccination debate in Twitter. Soc Media Soc2019;5:2056305119865465doi:10.1177/2056305119865465OpenUrlCrossRef↵Ginossar T, Shah SFA, Weiss DWalter D, Ophir Y. Online foreign propaganda campaigns and vaccine misinformation: a comparative analysis. In: Ginossar T, Shah SFA, Weiss D, eds. Vaccine Communication Online.Palgrave Macmillan, 2023, https://doi-org.ezproxy.cul.columbia.edu/10.1007/978-3-031-24490-2_6doi:10.1007/978-3-031-24490-2_6OpenUrlCrossRef↵Limaye RJ, Holroyd TA, Blunt M, et al. Social media strategies to affect vaccine acceptance: a systematic literature review. Expert Rev Vaccines2021;20:959-73. doi:10.1080/14760584.2021.1949292 pmid:34192985OpenUrlCrossRefPubMed↵Omer SB, Benjamin RM, Brewer NT, et al. Promoting COVID-19 vaccine acceptance: recommendations from the Lancet Commission on Vaccine Refusal, Acceptance, and Demand in the USA. Lancet2021;398:2186-92. doi:10.1016/S0140-6736(21)02507-1 pmid:34793741OpenUrlCrossRefPubMed↵Kahan D. Fixing the communications failure. Nature2010;463:296-7. doi:10.1038/463296a pmid:20090734OpenUrlCrossRefPubMedWeb of Science↵Ajeigbe O, Arage G, Besong M, et al., Stellenbosch Institute for Advanced Study African Scholars Network. Culturally relevant COVID-19 vaccine acceptance strategies in sub-Saharan Africa. Lancet Glob Health2022;10:e1090-1. doi:10.1016/S2214-109X(22)00251-0 pmid:35691328OpenUrlCrossRefPubMed↵Richard-Eaglin A, McFarland ML. Applying cultural intelligence to improve vaccine hesitancy among black, indigenous, and people of color. Nurs Clin North Am2022;57:421-31. doi:10.1016/j.cnur.2022.04.008 pmid:35985729OpenUrlCrossRefPubMed↵Papachrisanthou MM, Lorenz RA, Loman DG. Increasing immunization adherence among infants of low-income parents: the effects of visually enhanced education. J Nurse Pract2016;12:304-10doi:10.1016/j.nurpra.2015.12.021OpenUrlCrossRef↵Taba M, Ayre J, Freeman B, McCaffery K, Bonner C. COVID-19 messages targeting young people on social media: content analysis of Australian health authority posts. Health Promot Int2023;38:daad034. doi:10.1093/heapro/daad034 pmid:37099680OpenUrlCrossRefPubMed↵Thompson EL, Preston SM, Francis JKR, et al. Social media perceptions and internet verification skills associated with human papillomavirus vaccine decision-making among parents of children and adolescents: cross-sectional survey. JMIR Pediatr Parent2022;5:e38297. doi:10.2196/38297 pmid:36103216OpenUrlCrossRefPubMed↵Shen AK, Browne S, Srivastava T, Kornides ML, Tan ASL. Trusted messengers and trusted messages: the role for community-based organizations in promoting COVID-19 and routine immunizations. Vaccine2023;41:1994-2002. doi:10.1016/j.vaccine.2023.02.045 pmid:36803894OpenUrlCrossRefPubMed↵Hernandez RG, Hagen L, Walker K, O’Leary H, Lengacher C. The COVID-19 vaccine social media infodemic: healthcare providers’ missed dose in addressing misinformation and vaccine hesitancy. Hum Vaccin Immunother2021;17:2962-4. doi:10.1080/21645515.2021.1912551 pmid:33890838OpenUrlCrossRefPubMed↵Stecula DA, Kuru O, Jamieson KH. How trust in experts and media use affect acceptance of common anti-vaccination claims. Harv Kennedy Sch Misinformation Rev2020; doi:10.37016/mr-2020-007OpenUrlCrossRef↵US Centers for Disease and Prevention. About the vaccine conversations with parents campaign. 2019. https://www.cdc.gov/vaccines/hcp/conversations/about-vacc-conversations.html.↵National Academies. Communication strategies for building confidence in covid-19 vaccines: addressing variants and childhood vaccinations. https://nap.nationalacademies.org/catalog/26361/communication-strategies-for-building-confidence-in-covid-19-vaccines-addressing.↵Athey S, Grabarz K, Luca M, Wernerfelt N. Digital public health interventions at scale: The impact of social media advertising on beliefs and outcomes related to COVID vaccines. Proc Natl Acad Sci U S A2023;120:e2208110120. doi:10.1073/pnas.2208110120 pmid:36701366OpenUrlCrossRefPubMed↵Argyris YA, Nelson VR, Wiseley K, Shen R, Roscizewski A. Do social media campaigns foster vaccination adherence? A systematic review of prior intervention-based campaigns on social media. Telemat Inform2023;76:101918. doi:10.1016/j.tele.2022.101918 pmid:36438457OpenUrlCrossRefPubMed↵Sah P, Vilches TN, Moghadas SM, et al. Return on investment of the covid-19 vaccination campaign in New York City. JAMA Netw Open2022;5:e2243127. doi:10.1001/jamanetworkopen.2022.43127 pmid:36409495OpenUrlCrossRefPubMed↵Knudsen J, Perlman-Gabel M, Uccelli IG, Jeavons J, Chokshi DA. Combating misinformation as a core function of public health. NEJM Catal2023;4doi:10.1056/CAT.22.0198. OpenUrlCrossRef↵Ruggeri K, Palacios K, Perkins ZA, et al. Role of military forces in the New York State response to covid-19. JAMA Health Forum2022;3:e222136. doi:10.1001/jamahealthforum.2022.2136 pmid:36218979OpenUrlCrossRefPubMed↵Gallup. Confidence in institutions. 2007. https://news.gallup.com/poll/1597/Confidence-Institutions.aspx.↵New York State Department of Health. New York State’s covid-19 vaccination program. 2020. https://www.governor.ny.gov/sites/default/files/atoms/files/NYS_COVID_Vaccination_Program_Book_10.16.20_FINAL.pdf↵Lewandowsky S, Cook J, Lombardi D. Debunking handbook 2020. 2020. https://digitalcommons.unl.edu/scholcom/245/.↵Ecker UKH, Sharkey CXM, Swire-Thompson B. Correcting vaccine misinformation: A failure to replicate familiarity or fear-driven backfire effects. PLoS One2023;18:e0281140. doi:10.1371/journal.pone.0281140 pmid:37043493OpenUrlCrossRefPubMed↵Chan MS, Albarracín D. A meta-analysis of correction effects in science-relevant misinformation. Nat Hum Behav2023;7:1514-25. doi:10.1038/s41562-023-01623-8 pmid:37322236OpenUrlCrossRefPubMed↵Ghezzi P, Bannister PG, Casino G, et al. Online information of vaccines: information quality, not only privacy, is an ethical responsibility of search engines. Front Med (Lausanne)2020;7:400. doi:10.3389/fmed.2020.00400 pmid:32850905OpenUrlCrossRefPubMed↵Xin M, Luo S, Wang S, et al. The roles of information valence, media literacy and perceived information quality on the association between frequent social media exposure and covid-19 vaccination intention. Am J Health Promot2023;37:189-99. doi:10.1177/08901171221121292 pmid:35972385OpenUrlCrossRefPubMed↵Hughes CT, et al. Designing and implementing an educational social media campaign to increase HPV vaccine awareness among men on a large college campus. Am J Health Educ2020;51:87-97doi:10.1080/19325037.2020.1722297OpenUrlCrossRef↵Gursoy D, Ekinci Y, Can AS, Murray JC. Effectiveness of message framing in changing COVID-19 vaccination intentions: Moderating role of travel desire. Tour Manag2022;90:104468. doi:10.1016/j.tourman.2021.104468 pmid:34898791OpenUrlCrossRefPubMed↵Faccin M, Gargiulo F, Atlani-Duault L, Ward JK. Assessing the influence of French vaccine critics during the two first years of the COVID-19 pandemic. PLoS One2022;17:e0271157. doi:10.1371/journal.pone.0271157 pmid:35925962OpenUrlCrossRefPubMed↵Wang D, Qian Y. Echo chamber effect in rumor rebuttal discussions about covid-19 in China: social media content and network analysis study. J Med Internet Res2021;23:e27009. doi:10.2196/27009 pmid:33690145OpenUrlCrossRefPubMed↵Müller J, Tellier A, Kurschilgen M. Echo chambers and opinion dynamics explain the occurrence of vaccination hesitancy. R Soc Open Sci2022;9:220367. doi:10.1098/rsos.220367 pmid:36312563OpenUrlCrossRefPubMed↵Kozyreva A, Herzog SM, Lewandowsky S, et al. Resolving content moderation dilemmas between free speech and harmful misinformation. Proc Natl Acad Sci U S A2023;120:e2210666120. doi:10.1073/pnas.2210666120 pmid:36749721OpenUrlCrossRefPubMed↵IPIE. Platform responses to misinformation: a meta-analysis of data. Jul 2023. https://www.ipie.info/research/sr2023-2.↵Aubin CS, Liedke J. Most Americans favor restrictions on false information, violent content online. Pew Research Centerhttps://www.pewresearch.org/short-reads/2023/07/20/most-americans-favor-restrictions-on-false-information-violent-content-online/.↵Gavi, Unicef, World Health Organization, Vaccination Demand Hub, Health Enabled. Social listening: finding the signal through the noise. https://www.who.int/news/item/18-08- 2021-social-listening-finding-the-signal-through-the-noise. https://www.gavi.org/sites/default/files/2021-06/Finding-the-Signal-Through-the-Noise.pdf
Scientific evidence regularly guides policy decisions1, with behavioural science increasingly part of this process2. In April 2020, an influential paper3 proposed 19 policy recommendations (‘claims’) detailing how evidence from behavioural science could contribute to efforts to reduce impacts and end the COVID-19 pandemic. Here we assess 747 pandemic-related research articles that empirically investigated those claims. We report the scale of evidence and whether evidence supports them to indicate applicability for policymaking. Two independent teams, involving 72 reviewers, found evidence for 18 of 19 claims, with both teams finding evidence supporting 16 (89%) of those 18 claims. The strongest evidence supported claims that anticipated culture, polarization and misinformation would be associated with policy effectiveness. Claims suggesting trusted leaders and positive social norms increased adherence to behavioural interventions also had strong empirical support, as did appealing to social consensus or bipartisan agreement. Targeted language in messaging yielded mixed effects and there were no effects for highlighting individual benefits or protecting others. No available evidence existed to assess any distinct differences in effects between using the terms ‘physical distancing’ and ‘social distancing’. Analysis of 463 papers containing data showed generally large samples; 418 involved human participants with a mean of 16,848 (median of 1,699). That statistical power underscored improved suitability of behavioural science research for informing policy decisions. Furthermore, by implementing a standardized approach to evidence selection and synthesis, we amplify broader implications for advancing scientific evidence in policy formulation and prioritization. Evaluation of evidence generated to test 19 proposed policy recommendations and guidance for the future.
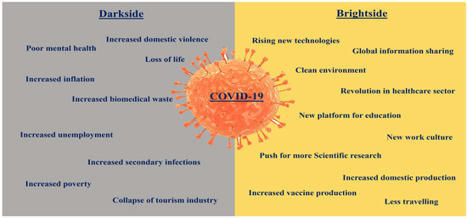
On 5 May 2023, the World Health Organization (WHO) officially declared the end of the coronavirus disease-19 (or COVID-19) pandemic. Even before the official announcement from the WHO, signs of recovery from the pandemic started appearing, especially after rapid worldwide vaccination.
|
This study examined the public’s sentiments about vaccines by analyzing Twitter data during the CDC’s vaccination management planning stage in the United States. Sentiment scores were assigned to each tweet using a sentiment dictionary and the sentiment changes were analyzed over 52 weeks from...
Identifying determinants of vaccination uptake is critical for public and community health. The population became divided in regard to preventative measures and vaccinations during the COVID-19 pandemic.
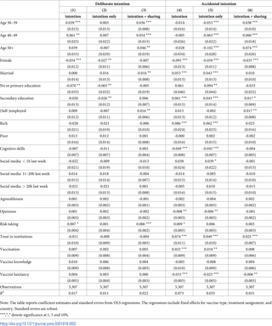
The widespread dissemination of misinformation on social media is a serious threat to global health. To a large extent, it is still unclear who actually shares health-related misinformation deliberately and accidentally.
Prior research identifies trust as critical to increase vaccine acceptance and uptake. However, few intervention studies have sought to develop or test strategies for bolstering vaccine-related trust.
Widespread acceptance of a vaccine for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) will be the next major step in fighting the coronavirus disease 2019 (COVID-19) pandemic, but achieving high uptake will be a challenge and may be impeded by online misinformation. To inform successful vaccination campaigns, we conducted a randomized controlled trial in the UK and the USA to quantify how exposure to online misinformation around COVID-19 vaccines affects intent to vaccinate to protect oneself or others. Here we show that in both countries—as of September 2020—fewer people would ‘definitely’ take a vaccine than is likely required for herd immunity, and that, relative to factual information, recent misinformation induced a decline in intent of 6.2 percentage points (95th percentile interval 3.9 to 8.5) in the UK and 6.4 percentage points (95th percentile interval 4.0 to 8.8) in the USA among those who stated that they would definitely accept a vaccine. We also find that some sociodemographic groups are differentially impacted by exposure to misinformation. Finally, we show that scientific-sounding misinformation is more strongly associated with declines in vaccination intent. A randomized controlled trial reveals that exposure to recent online misinformation around a COVID-19 vaccine induces a decline in intent to vaccinate among adults in the UK and the USA.
The main objective of this study was to determine whether one of the most commonly employed pro-vaccination strategies based on the “myths vs. facts” format can be considered an effective tool to counter vaccines misinformation. Sixty parents were randomly presented with either a control message or a booklet confronting some common myths about vaccines with a number of facts. Beliefs in the autism/vaccines link and in vaccines side effects, along with intention to vaccinate one’s child, were evaluated both immediately after the intervention and after a 7-day delay to reveal possible backfire effects. Data provided support for the existence of backfire effects associated with the use of the myths vs. facts format, with parents in this condition having stronger vaccine misconceptions over time compared with participants in the control condition. The myths vs. facts strategy proved to be ineffective. Efforts to counter vaccine misinformation should take into account the many variables that affect the parents’ decision-making.
A journal is retracting a paper on the purported harms of vaccines against COVID-19 written in part by authors who have had similar work retracted before. The article, “COVID-19 mRNA Vaccines: Lessons Learned from the Registrational Trials and Global Vaccination Campaign,” appeared late last month in Cureus, which used to be a stand-alone journal but…
Objectives France and Germany have different approaches towards childhood immunisation. The aim of this study was to determine the similarities and differences between France and Germany in terms of heath policies, vaccination rates and public opinion as far as infant vaccinations were concerned. Study design Literature review. Subject and methods We used the databases of the Robert Koch Institute (RKI) and of Santé publique France (SpF) to compare the vaccination rates of children in the year 2017. The state of public opinion was principally assessed by comparing data from SpF and the German Federal Center for Health Education (BZgA). Results Vaccination rates were higher in French pre-school children in 2017 for the hexavalent and anti-pneumococcal vaccines, whereas Measles–Mumps–Rubella and anti-meningococcal vaccination rates were higher in Germany. Public opinion was more favourable towards vaccines in Germany than in France. Some vaccines, especially against seasonal influenza and hepatitis B, were viewed with criticism in France, whereas German parents considered hepatitis B immunisation to be important for their children. Moreover, both countries showed higher immunisation rates in northern regions. This correlated with the state of vaccine confidence in France. In Germany, eastern regions were more favourable towards vaccines, which correlated with higher immunisation rates in these regions. Conclusions The state of vaccine confidence seemed to correlate with immunisation rates in both countries. The need for information about vaccines is still high in both countries and trust in the medical community as well as in the immunisation policymakers should be reinforced as a priority.
À l’occasion de l’examen de la loi sur les fake news, qui débute au Parlement ce jeudi 7 juin 2018, The Conversation France a décidé – en partenariat avec le centre de recherche de l’université de Lorraine, le CREM – de compiler une sélection de leurs meilleurs articles sur cette thématique, afin...
WHAT IS ALREADY KNOWN ON THIS TOPICAvailable literature has demonstrated an association between the level of public trust in scientists and adherence to protective behaviours during epidemics and has emphasised the importance of effective public health communication to ensure compliance with public health guidance.WHAT THIS STUDY ADDSThe present study found that the distrusting public sought to ‘outscience’ the scientists, questioned who was a ‘scientist’, and contended that political and economic interests controlled scientific inquiry. Definitions of ‘scientists’ and ‘scientific investigation’ and perceived roles of scientists in epidemic emergence and policymaking are more varied than prior research presumed. Our study thus extends knowledge about trust in scientists by questioning assumptions about public definitions of ‘scientist’ and ‘scientific investigation’.HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICYThis study expands the scope of research on trust in scientists by investigating qualitatively public understanding and definitions of scientists, scientific investigation and uncertainty. These insights should be integrated into strengthening scientific literacy in Europe.IntroductionPreoccupations with public trust in scientists and science are not new.1 Longitudinal and multicountry surveys have assessed public confidence in science and scientists, in relation to sociodemographic factors such as age, gender, education level and political affiliation.2 3 Other studies have investigated specific factors affecting public trust in science and scientists, including perceived transparency, belief in pseudoscience,4 trust in government and corporations,5 conflicts of interest6 and historical cases of misuse of biomedical research.7 The COVID-19 pandemic accentuated public health specialists’ concerns about public trust in science and scientists,8 9 particularly because this trust is so closely linked to adherence to preventive measures, both non-pharmaceutical and vaccination.10 11 Past and current assessments of public trust in scientists and science have delineated similar profiles of social groups more or less likely to trust.10–12 Since 2020, they have also identified the global proliferation of controversies around pandemic origins, non-pharmaceutical interventions, vaccines and treatments.13 Facilitated by social media platforms and widespread anxiety in the recent pandemic crisis, certain social groups have been characterised as governed by emotion,14 irrationality,15 overconfidence16 and ignorance.17 Underpinning these studies addressing trust in scientists and science is an assumption that ‘scientists’ constitute a cohesive, homogeneous community engaged in a consensus-driven pursuit of knowledge.Dissent, however, is at the core of scientific endeavour,18 and it is crucial for producing consensus, which is often fleeting.19 The profound uncertainties and debates characterising the scientific understanding of SARS-CoV-2, COVID-19, and prevention and treatment measures mirror the dissent that Thomas Kuhn found so fundamental to the production of scientific knowledge. In his seminal work ‘The Structure of Scientific Revolutions’, Kuhn argued that scientific progress is not always linear or cumulative. Instead, it often entails ‘paradigm shifts’, in which persistent anomalies and dissenting views challenge established frameworks of understanding, catalysing their replacement by new frameworks. The profound uncertainties and debates surrounding SARS-CoV-2, COVID-19, and its prevention and treatment measures provoked such Kuhnian debates and changing frameworks. Uncertainty during the pandemic also generated public health measures based on what Eysenbach20 has described as the ‘best available evidence’, and not ‘evidence-based facts’. Two salient questions remain unexplored in the literature on trust in science and scientists. First, proliferating surveys about public ‘trust in scientists’ and ‘trust in science’ without deeper exploration of lay understanding of who qualifies as a scientist and what scientists do misrepresent the complex and contentious processes of scientific knowledge production, particularly in uncertain and volatile epidemic contexts. We need better insight into the public’s understanding of what constitutes science, who can be considered a scientist and scientists’ roles—or lack thereof—in epidemic policymaking and response. Second, although numerous studies have examined levels of confidence towards science or scientists among different social and demographic groups, as well as associations between this trust and specific non-sociodemographic factors, there is scarce exploration and analysis of why the diverse public trust or distrust science and scientists.We therefore conducted a cross-sectional mixed-methods survey among 7000 respondents in seven European countries (Belgium, France, Germany, Italy, Spain, Sweden and Ukraine) to investigate public trust in scientists engaged in COVID-19 research. Conducted in December 2020, the survey occurred at a crucial historical moment for public trust in scientists, when news of an effective COVID-19 vaccine had just been announced and plans for vaccine rollout were under way. The survey sought to identify diverse factors linked to the public trust in scientists involved in COVID-19 research, but also queried participants through closed-ended questions and text boxes about their understanding of pandemic origins and intentions to accept vaccination or specific treatments for COVID-19. Open-text responses revealed much about the public understanding of who are scientists, the work they do, the claims and practices they consider to be scientific, and the roles they and other actors have in producing knowledge to inform pandemic response.MethodsTo develop the cross-sectional mixed-methods survey, we carried out social listening (online collection and analysis) of COVID-19-related tweets in English posted by users in the European Union in May–June 2020. We employed thematic coding to identify ongoing scientific controversies, top narratives circulating about scientists, trials, vaccines and treatments, including conspiracy-related discourses. We then used the results to create a survey investigating trust in scientists and in national and international authorities and institutions and included questions about the understanding of pandemic origins, and anticipated protective practices and devices, and treatment.The cross-sectional survey, conducted by the market research firm Ipsos, was implemented through an online survey on 4–16 December 2020 among 7000 respondents in Belgium, France, Germany, Italy, Spain, Sweden and Ukraine. Following its standard protocol, Ipsos set quotas aligned with nationally representative proportions based on age (18–65 years), gender, geographical region and working status for each country. Ipsos developed a sample of participants from its existing online research panels, contacting potential participants by email to participate. When each quota was filled, Ipsos closed the quota immediately. One thousand respondents between 18 and 65 years old in each country participated. Ipsos did not survey those over age 65 years because its panel surveys cannot ensure representative sampling of this population. The following quantitative data were collected among respondents: socioeconomic and demographic characteristics, including gender identification (male/female/other/prefer not to answer); trust in sources of medical and scientific information; trust in national, European, and international institutions and authorities, as well as in pharmaceutical companies; perception of vaccine contents, purposes and safety; and political affiliation. The questionnaire included questions about participant understanding of clinical trials, perceptions of COVID-19 origins, prevention, testing, treatment preferences and anticipated COVID-19 vaccine acceptance. Trust in scientists was defined based on participants’ responses to three questions in the survey. Participants were asked to rank their level of agreement to the following statements:‘Scientists working in my country are competent to do research on COVID-19.’‘Scientists working in my country who are doing research on COVID-19 would be honest about what they discover.’‘Scientists working in my country who are doing research on COVID-19 are doing their work in the best interests of the public.’Data analysisData analyses were quantitative and qualitative. We initially conducted descriptive statistical analyses, presenting categorical variables as N (number of participants) and % (percentage from the total study population) for each category of variable. For analysis of trust, we combined the three questions above on trust into a single binary variable (trust/no trust), which served as a proxy to reflect trust in scientists. Relationships between trust in scientists and other factors (sociodemographic, information sources, personal COVID-19 experiences and beliefs in specific rumours) were analysed using an Akaike Information Criterion-based stepwise backwards multivariate regression model. We used France as the reference class. All results are expressed as ORs and 95% CIs. All quantitative analyses were performed using R software V.4.1.1.Survey participants’ open-text responses about COVID-19 treatment, vaccination and SARS-CoV-2 origins were evaluated using thematic analysis.21 We developed a global codebook and conducted inductive and deductive thematic coding using NVivo software (QSR international, V.1.7.1). We also organised our analyses to categorise descriptions of existing COVID-19 scientific research according to expressed trust in scientists, participant sentiments towards key actors and explanations of responses contending that SARS-CoV-2 was deliberately released. Blank (unanswered) text boxes were not evaluated.To ensure high-quality text analysis, a native speaker of each country language (French, Italian, Spanish, Ukrainian, German, Flemish and Swedish) performed the coding. All coders conferred frequently during the coding process to address and compare transversal codes and themes.Patient and public involvementThere were no patients involved in the study. We did not explicitly involve the public in the research questions, design, recruitment or outcome measures of the study, nor were they asked to assess the burden of time required to participate in the research. Our development of the survey tool, however, did draw on specific debates about COVID-19 on Twitter.ResultsQuantitative resultsOur sample exhibited a balanced distribution of gender and age groups. In this sample, 34% participants were not employed, 43% identified as having centrist political beliefs and most possessed at least secondary education (see online supplemental file 1).Supplemental material[bmjph-2023-000280supp001.pdf]Table 1 evaluates trust in scientists and its associations with sociodemographic characteristics, use of information sources and beliefs, and experiences with COVID-19. Statistically significant associations were observed between trust in scientists and sociodemographic characteristics (country of origin, age, level of education, political affiliation). In comparison with France, respondents residing in Belgium (OR 1.25, 95% CI 1.03 to 1.52, p<0.025), Italy (OR 1.26, CI 1.04 to 1.54, p<0.020) and Sweden (OR 1.41, CI 1.16 to 1.72, p<0.001) had higher odds of trusting scientists. In contrast, respondents in Germany (OR 0.79, CI 0.65 to 0.96, p=0.018) and Ukraine (OR 0.39, CI 0.31 to 0.49, p<0.001) were less trustful of scientists. In comparison with the youngest respondents (18–24 years old), older groups, notably those 44–54 years old (OR 1.36, CI 1.12 to 1.65, p=0.002) and 55–65 years old (OR 1.71, CI 1.41 to 2.08, p<0.001), expressed significantly more trust in scientists. Participants with secondary (OR 1.33, CI 1.05 to 1.70, p=0.018) and tertiary (OR 1.57, CI 1.24 to 1.99, p<0.001) education levels also tended to trust scientists more than those with only primary education. Those declaring a preference to vote for centre (OR 1.15, CI 1.01 to 1.32, p=0.041) and left (OR 1.59, CI 1.33 to 1.89, p<0.001) political parties showed higher levels of trust than those affiliating themselves with politically right-wing parties.View inline View popup Table 1 Relations between sociodemographic characteristics, information sources and beliefs, experience with COVID-19 and trust in scientistsUse of certain information sources about COVID-19 was also significantly associated with trust in scientists. Participants obtaining their information via traditional media (newspapers, TV, radio, etc) (OR 1.48, CI 1.28 to 1.72, p<0.001), mainstream organisational/institutional websites (OR 1.39, CI 1.24 to 1.55, p<0.001), face-to-face discussions with friends and family (OR 1.15, CI 1.02 to 1.30, p=0.016) and their healthcare environment (eg, posters in hospital waiting rooms) (OR 1.23, CI 1.07 to 1.43, p=0.005) trusted in scientists more than those who did not. Respondents who reported seeking COVID-19-related information from blogs and non-mainstream websites (OR 0.81, CI 0.68 to 0.97, p=0.024), online conversations (OR 0.84, CI 0.72 to 0.97, p=0.016) and those who stated they did not use any information sources listed in the survey (OR 0.62, CI 0.40 to 0.94, p=0.027) were less trustful of scientists than those who did not.Experience with COVID-19 was also associated with trust in scientists, including having a close family member or friend with COVID-19-like symptoms (OR 1.18, CI 1.03 to 1.35, p=0.017) or knowing someone who had been in an intensive care unit (ICU) due to COVID-19 (OR 1.21, CI 1.01 to 1.44, p=0.038). In addition, not knowing someone admitted to an ICU also yielded higher odds of trusting scientists (OR 1.24, CI 1.08 to 1.42, p=0.002).Embracing narratives that significantly deviated from mainstream scientific debates about SARS-CoV-2 origins and purported roles of certain technologies in COVID-19 was significantly associated with decreased trust in scientists. Participants contending that COVID-19 was deliberately released from a laboratory (OR 0.43, CI 0.37 to 0.50, p<0.001) and that COVID-19 symptoms worsened with exposure to 5G technology (OR 0.53, CI 0,37 to 0.75, p<0.001) had much lower odds of trusting scientists than those indicating that they did not believe in these rumours.The distribution of responses to COVID-19 origins and aggravators differed across countries, as shown in figure 1. In all countries except Ukraine, respondents most frequently attributed the pandemic origin to a zoonotic spillover. In Ukraine, however, respondents most frequently selected the response that the pandemic resulted from a deliberate viral release. Across all countries, at least one-third of respondents believed that the virus was accidentally or deliberately released. Claims that COVID-19 symptoms are caused or worsened by 5G technology were rare in all countries.<img src="https://bmjpublichealth.bmj.com/content/bmjph/1/1/e000280/F1.medium.gif"; class="highwire-fragment fragment-image" width="440" alt="Figure 1" height="255">Download figure Open in new tab Download powerpoint Figure 1 COVID-19 origins and aggravators by country.Table 2 shows that participants trusting scientists were more likely to believe that the COVID-19 pandemic origins resulted from a zoonotic spillover (OR 2.82, CI 2.55, 3.12, p<0.001) and to accept a COVID-19 vaccine (OR 3.67 OR, CI 3.29, 4.09, p<0.001). The relationship between trust in scientists and acceptance of paracetamol, the sole recommended treatment at the time, was not statistically significant (OR 1.1, CI 0.89, 1.35, p=0.4).View inline View popup Table 2 Perceptions of COVID-19 origins and anticipated vaccine or paracetamol treatment acceptance among respondents trusting scientistsQualitative resultsOur qualitative results centred on text responses to queries about pandemic origins, intentions to accept specific COVID-19 treatments and anticipated COVID-19 vaccine acceptance. Overall, participants provided a total of 8404 open-text responses explaining their theories of pandemic origins (1859 responses) and intentions to accept a specific COVID-19 treatment (2205 responses) and a COVID-19 vaccine (4340 responses) (online supplemental file 2).Supplemental material[bmjph-2023-000280supp002.pdf]Roughly equal numbers of respondents trusting and not trusting scientists frequently referred to scientific research to justify their responses to questions about COVID-19 origins and intentions to accept COVID-19 vaccination and paracetamol as COVID-19 treatment (table 3). Participants also signalled a lack of data to support claims about treatments and vaccines. Those not trusting scientists tended to claim that existing knowledge was insufficient or that more research was needed. Crucially, these respondents mobilised apparently scientific justifications to support their contentions. One participant denying the pandemic’s cause was a zoonotic spillover argued, ‘No link established for animal transmission to date; ‘surprising’ viral sequence…’View inline View popup Table 3 Trust in scientists and descriptions of existing COVID-19 scientific researchRespondents not trusting scientists expressed roughly equally positive and negative comments about scientists (online supplemental file 3). Those not trusting scientists sometimes underscored scientists’ prowess to support their own convictions the virus was released intentionally. Still others lauded certain researchers who have taken stances against the dominant scientific discourse, notably Didier Raoult, who claimed that hydroxychloroquine was an effective COVID-19 treatment, and Franco Trinca, who advocated ‘free choice’ regarding COVID-19 vaccine uptake. Both Raoult (French dataset) and Trinca (Italian dataset) were applauded for their willingness to treat patients with drugs not recommended by national authorities (ie, hydroxychloroquine). Another respondent cited a ‘Nobel prize winner’ as a source for the claim that SARS-CoV-2 was not a ‘natural’ virus. Participants trusting scientists responded somewhat more positively about scientists but mentioned no individual scientists in their responses. Few scientists were named and applauded for their merits, but those mentioned had all challenged mainstream scientific discourses about COVID-19 origins and treatments.Supplemental material[bmjph-2023-000280supp003.pdf]Many respondents, although neither lauding or attacking scientists, suggested that scientists themselves were powerless, serving instead more powerful actors, including states, economic interests and pharmaceutical companies. Such reflections appeared in claims that scientists had developed COVID-19 vaccines long before the pandemic for authorities or had inserted microchips to control populations in these vaccines.Even more revealing were open-text responses concerning pandemic origins, showing scientists as neither the most cited nor the most significant actors. Among participants contending that SARS-CoV-2 was deliberately released, we identified four themes in all country respondents (table 4). First, some respondents argued that the deliberate viral release was to impose demographic control, to reduce elderly and poor populations, and thus to decrease public spending on pensions, healthcare or social welfare. A second theme contended that the pandemic bolstered a country’s geopolitical standing. A French respondent, for instance, designated China as the cause of the pandemic, waging ‘a war without arms, aimed at weakening Europe and the U.S.’. China was the focus of much criticism (see also online supplemental file 3), with respondents contending that Chinese authorities had deliberately released the virus as part of its geopolitical strategy. Third, respondents argued the deliberate viral release was designed to reap financial benefits. A Ukrainian respondent contended that the pandemic was a means ‘to cause the final collapse in third world countries and further manipulate them for their own enrichment. Western European countries, the United States and China are enriching themselves.’ An Italian participant saw the beneficiaries as more circumscribed, arguing: ‘Behind every world catastrophe there is always a small circle of people … beyond nationality, ethnicity and government office…who make a huge profit at the expense of the general community’. Participants not trusting scientists were highly critical of pharmaceutical companies, arguing that these companies had deliberately released the pandemic virus to profit from vaccines. Finally, respondents contended that governments or ‘politicians’ released the virus to increase control over citizens. Another Italian participant observed, ‘The scoop is to further the Great Reset and create an Orwellian-style dictatorial world through the excuse of the pandemic’. A handful of participants offered other explanations, which were too diffuse or unclear to categorise.View inline View popup Table 4 Frequency (Freq) of most common narratives in open-text responses about deliberate COVID-19 releaseAlthough these narratives appeared in all seven countries, their prevalence varied (see table 4). Open-text responses in Belgium, France and Ukraine highlighted demographic control as an explanation for the virus’s deliberate release, whereas Italy and Sweden tended to highlight its release as generating geopolitical advantages to other countries.DiscussionThe present study investigated factors associated with European public trust in scientists at a crucial moment in the COVID-19 pandemic, exploring text responses concerning COVID-19 origins and intentions to accept COVID-19 treatments and vaccines. Our findings indicate higher levels of trust in scientists within higher-income countries of Belgium, Italy and Sweden, and less trust in Ukraine, a lower-income country. Consistent with previous research,22 23 we observed higher trust among older individuals, those in higher-income countries and those with higher educational levels. In contrast to a Wellcome Trust study,22 we found greater trust among respondents over 45 years old.Political affiliation appears to play a role in trust levels. Our study suggests that those aligned with the political left and centre exhibited greater trust in scientists compared with their right-leaning counterparts, aligning with trends observed in the USA and Europe, where public perceptions of science have been influenced by political discourse.24 25 In contrast, one German study examining changing levels of trust in science over the pandemic reported that trust increased at its outset but declined over time, more so among right-wing voters.Health information sources also influenced participants’ trust of scientists. Participants who used print and online newspapers, magazines, television, radio, news websites or apps, websites of mainstream organisations, as well as those who obtained information through personal conversations with friends and family or from healthcare environment trust scientists in their countries more than those who do not. Our findings differ from a broader literature on information sources during the COVID-19 pandemic, which have not addressed correlations with trust in scientists.26Participants’ direct experience with COVID-19 (close contact with COVID-19-like symptoms or knowing someone who had been in an ICU), as well as not knowing someone admitted to an ICU for COVID-19, were positively associated with trust in scientists. These apparently contradictory findings, and particularly not knowing someone admitted to an ICU, could have resulted from the large sample size leading to more variables being statistically significant.This study also found that beliefs in conspiracy-related narratives—that the pandemic resulted from a deliberate release of SARS-CoV-2 and that 5G technology exacerbated COVID-19 symptoms—were associated with lower levels of trust in scientists. Similarly, previous studies reported that belief in conspiracy theories was negatively associated with public trust in science27 and adoption of protective behaviours.28 The emergence and circulation of conspiracy narratives (beliefs that ‘major public events are secretly orchestrated by powerful and malevolent entities acting in concert’26) and an infodemic (a plethora of correct and incorrect health information) have been crucial features of this pandemic.20 29 30Our analyses of open-text responses effectively recast our questions about public trust in scientists. First, we found that both respondents trusting and distrusting scientists supported their claims by citing existing scientific research and expressed a need for additional scientific data and research. These results suggest that respondents—even those not trusting national scientists—sought to employ evidence-based thinking. This finding appears to counter claims that those not trusting mainstream scientific discourse act out of emotion or irrationality.15 Although this question requires further investigation, our results suggest that scepticism of existing scientific knowledge on the eve of COVID-19 vaccine rollout in Europe fuelled demands for more scientific evidence. Whereas physicist Edwin Hubble31 argued that ‘a healthy dose of scepticism’ is a prerequisite to scientific thinking, European respondents in this study were highly sceptical of expert judgement. Although Atul Gawande indicates that a scientific mindset ‘observe[s] the world with an open mind, gathering facts and testing […] predictions and expectations against them’,32 distrustful participants in the present study signalled that they undertook similar approaches: they cited published works, they gathered observations, although anecdotal, but ones they considered to be facts. Appropriating this sceptical stance and scientific processes, respondents not trusting mainstream scientists across all surveyed countries suggests a desire to ‘outscience’ the scientists.For Feinstein,33 laypeople are outsiders to science; they rely on scientific knowledge communicated to them. This outsider status uncovers a deep paradox of trust in science: the promise of modern science is to ‘know the truth instead of just trusting what you are told’, and yet trust in science is equally essential, when laypeople cannot surmount barriers of highly specialised, complex scientific knowledge.34 The information revolution once raised hopes for greater public participation in science,19 but new concerns about a post-truth era35 have displaced these earlier aspirations. Still, some respondent efforts to ‘outscience’ the scientists may reflect a continued desire to engage more fully in scientific investigation and findings, to discover truth for themselves. Respondents’ clamours for more data may also result from a conscious strategy to set impossible standards of certainty, to generate doubts and to postpone decision-making about viral origins, vaccines or treatments. Proctor and Schiebinger have described a similar strategy among interest groups engaged in scientific controversies.36Second, our findings raised the question about who can be considered a scientist. Respondents who did not trust scientists in their own countries nevertheless appeared to mention and trust individuals whom they considered to be scientists, but who were controversial or whose status was disputed (eg, Raoult, Trinca). Some commentators have attributed lack of trust in science as the result of ‘fake experts […] who do not actually have a credible scientific track record’.32 Yet, individuals mentioned by respondents—even those roundly castigated by mainstream science for their records during the pandemic—remain difficult to dismiss as ‘fake experts’. Our results highlight the major challenges that the European public face in distinguishing ‘real’ from ‘fake’ scientists. A recent report, for instance, found that 65% of online anti-vaccine content originated with some 12 individuals; our further investigation into these individuals found that half declared that they possessed a medical or biomedical degree.37 The lay public may label active, influential critics as scientists, even when the latter disseminate inaccurate information in their online profiles, are banned from medical boards, or dismissed as pseudo-scientists in news outlets or peer-reviewed journals.Third, we found that the participants’ rationale concerning pandemic origins or plans for COVID-19 treatment or vaccination did not attribute central roles to scientists. Certain respondents appeared to assign more pivotal roles to states, politicians and pharmaceutical companies, suggesting that an intentional viral release would enable powerful actors to reduce certain populations and expenditures on healthcare or social support, or to benefit economically from vaccines. Although these narratives were marked by the absence of scientists, they implied that scientists were nonetheless carrying out agendas of more powerful actors. These results align with Harambam’s findings38 that online Dutch conspiracy narratives often challenge the image of science as a collective, impartial search for knowledge, and that ‘science’, particularly biomedical research, is corrupted by the corporate world.The four principal narratives identified in participants’ justifications for believing in the deliberate release of SARS-CoV-2—demographic control, geopolitical advantage, financial profit and social control—were observed across all countries, languages and cultural areas, although with varying intensities. That these narratives appeared across all country populations included in this survey suggest a shared cultural and linguistic ‘informational ecosystem’ across Europe.Conspiracy narratives, despite their fallacies, offer a window into the underlying anxieties of those believing and spreading them.39 Demographic control narratives were especially prevalent in countries with ageing populations highly affected by COVID-19 in December 2020, notably France, Belgium and Italy. These countries are currently grappling with debates over funding their social retirement systems and sustaining their models of social support. The geopolitical advantage narrative, attributing the pandemic to a Chinese attempt to undermine the West, appeared to resonate with populations anxious about the emergence of a multipolar world, in which Europe and the USA no longer dominate as global economic, cultural and military powers. Respondents from all countries evoked this narrative, but more frequently in Italy and Sweden. Finally, the financial profit and social control narratives, possibly alimented by fears of concentrated power in the hands of private and/or state actors, were somewhat more prominent in France and Italy, which in recent years have been preoccupied by debates over accumulation of wealth and power by these actors.All these narratives often align with and sometimes explicitly reference the Great Reset, a multifaceted conspiracy theory suggesting collusion between governments and large corporations to orchestrate the pandemic.40 Significantly, science and scientists do not feature prominently in such rationale. Scepticism or mistrust of science and scientists does not develop in a vacuum, but is produced and sustained by historical events that shape contemporary attitudes. Past abuses, such as the infamous Tuskegee Syphilis Study in the USA and the Mediator obesity drug scandal, demonstrate that unethical research practices and misapplications of scientific knowledge leave indelible traces on public memory, eroding long-term trust in science and scientists.41–43One singular feature of our study is that it employed an approach that was initially qualitative, then quantitative, then mixed. We first conducted a thematic analysis of online discourse (social listening), using this analysis of the infodemic to inform our survey questions, which integrated key quantitative measures and open-text answers. Quantitatively, we evaluated trust indicators, gauged the prevalence of prominent pandemic conspiracy beliefs, and assessed anticipated vaccine acceptance and treatment preferences. Subsequently, our qualitative analysis highlighted fluid definitions of what constitutes a scientist; the common practice of citing sources to support claims about pandemic origins among both trusting and distrusting participants; four principal themes (demographic control, geopolitical positioning, financial benefit and political control over citizens) that underlay distrustful attitudes towards scientists consistent across nations; and an in-depth mapping of trust dynamics among actors mentioned in participants’ open rationales.Mobilising and combining quantitative and qualitative methodologies leveraged the strengths of each approach. Upstream of the study, qualitative methods crucially highlighted previously unidentified variables through inductive characterisation of online discourse (social listening). These methods also contributed significantly to elucidating and analysing public explanations of their claims around pandemic origins and attitudes towards scientists. In turn, quantitative methods produced additional precision about key indicators of trust in scientists and associated factors and cross-country comparisons of predominant online discourses. Shuttling between and combining mixed-methods appear especially apt for analyses of rapidly changing, polarising and complex subjects like trust in scientists and science during an epidemic or pandemic.Limitations of the studyThis study has multiple limitations. First, because the survey was administered online, respondents with better computer and internet access and higher levels of education were more likely to be recruited and to participate. Moreover, because Ipsos survey panels do not include participants over 65 years old due to uneven internet knowledge and use, we were unable to collect and analyse responses from older populations, which would have been illuminating.Second, the survey was conducted over a 12-day period in December 2020, and in seven European countries. Our results are neither representative of all European countries, nor of high-income countries outside of Europe and middle-income and low-income countries (where populations may be less trustful of scientists). Trust in scientists may have changed significantly since December 2020. For this reason, our findings and conclusions are applicable to the seven European countries where the study was conducted. Although they reveal trust at a specific moment in the past, we employ these results to raise questions implicit in studies of trust in scientists and to encourage further investigation.In investigating factors associated with trust in scientists, the present research did not address trust in science more generally. The survey contained specific questions about scientists’ honestly, integrity and intention to act in the interest of the public. ‘Science’ is a broad term, encompassing multiple actors, processes and practices. We compare our results with studies addressing both trust in ‘scientists’ and ‘science’, although we recognise that these terms do not have the same meaning for respondents.The study’s large (N=7000) sample size in countries with diverse health, political, social, economic and cultural indicators, and conditions led to more statistically significant variables. A study of individual countries could shed additional light on more significant associations.Finally, not all respondents explained their responses in text boxes. It is possible that respondents more adamant about their claims were more likely to respond to these specific questions. That said, in a previous publication, we found that responses to questions about intention to accept COVID-19 vaccination expressed conditionality.44 We would suggest, then, that these responses reflect a broad range of opinions, and not just those more convinced of their claims.ConclusionThis mixed-methods study of trust in scientists study integrated quantitative multivariate analysis and thematic analysis of participants’ open-text rationale. It produced statistically significant results on drivers of trust in scientists among the public in seven European countries, but also identified a shared reliance on evidence-based thinking among participants who trust scientists and those who do not, the relative erasure of scientists from participants’ rationale in favour of other actors and the predominance of controversial scientists among individual scientists.These results should encourage additional investigation of trust in scientists beyond sociodemographic and other drivers, to explore public conceptions of scientists and of scientific investigation. They also should inform multipronged measures to enhance trust in scientists, which should include enhancing scientists’ visibility and emphasising their independence, as well as promoting greater public literacy about scientific investigation and uncertainty. Tackling the broader sociopolitical anxieties about public powerlessness in the face of powerful political and economic interests—which provide fodder for conspiracy narratives—may also indirectly strengthen trust in scientists.Although our findings offer important insight into the dynamics of trust in scientists across selected European countries, they also underscore complexity of this trust. Given its crucial implications for public health policy and communication strategies, more granular investigations of the sociocultural, historical factors influencing public trust at national level are needed. Further research can guide more effective and nuanced science communication in the future.Data availability statementData are available upon reasonable request.Ethics statementsPatient consent for publicationNot required.Ethics approvalThis study involves human participants and the University of Antwerp ethics committee provided ethical approval for all methods of the study, including the initial X (formerly Twitter) analysis (20/13/150). All participants furnished online informed consent before participating in the survey.References↵Mazur A. Public confidence in science. Soc Stud Sci 1977;7:123–5. doi:10.1177/030631277700700113OpenUrlCrossRef↵Gauchat G. Politicization of science in the public sphere: a study of public trust in the United States, 1974 to 2010. Am Sociol Rev 2012;77:167–87. doi:10.1177/0003122412438225OpenUrlCrossRefWeb of Science↵Eurobarometer S. European citizens’ knowledge and attitudes towards science and technology, 4. Eurobarometer, 2021.↵Lewandowsky S, Gignac GE, Oberauer K. The role of conspiracist Ideation and worldviews in predicting rejection of science. PLoS One 2013;8:e75637. doi:10.1371/journal.pone.0075637↵Pechar E, Bernauer T, Mayer F. Beyond political ideology: the impact of attitudes towards government and corporations on trust in science. Sci Commun 2018;40:291–313. doi:10.1177/1075547018763970OpenUrl↵Krimsky S. Science in the private interest: has the lure of profits corrupted biomedical research? Rowman & Littlefield, 2004: 276.↵Bates BR, Harris TM. The Tuskegee study of untreated Syphilis and public perceptions of BIOMEDICAL research: a focus group study. J Natl Med Assoc 2004;96:1051–64.OpenUrlPubMed↵Roundtable on Public Interfaces of the Life SBoard on Life SDivision on Eet al. Trust and confidence at the interfaces of the life sciences and society: does the public trust science? Trust and confidence at the interfaces of the life sciences and society: does the public trust science? A workshop summary. Washington (DC): National Academies Press (US),↵Eiser JR, Stafford T, Henneberry J, et al. "Trust me, I'm a scientist (not a developer)": perceived expertise and motives as predictors of trust in assessment of risk from contaminated land. Risk Anal 2009;29:288–97. doi:10.1111/j.1539-6924.2008.01131.xOpenUrlPubMed↵Algan Y, Cohen D, Davoine E, et al. Trust in scientists in times of pandemic: panel evidence from 12 countries. Proc Natl Acad Sci U S A 2021;118:e2108576118. doi:10.1073/pnas.2108576118↵Bajos N, Spire A, Silberzan L, et al. When lack of trust in the government and in scientists reinforces social inequalities in vaccination against COVID-19. Front Public Health 2022;10:908152. doi:10.3389/fpubh.2022.908152↵Sturgis P, Brunton-Smith I, Jackson J. Trust in science, social consensus and vaccine confidence. Nat Hum Behav 2021;5:1528–34. doi:10.1038/s41562-021-01115-7OpenUrl↵Calleja N, AbdAllah A, Abad N, et al. A public health research agenda for managing Infodemics: methods and results of the first WHO infodemiology conference. JMIR Infodemiology 2021;1:e30979. doi:10.2196/30979↵Bratu S. The fake news sociology of COVID-19 pandemic fear: dangerously inaccurate beliefs, emotional contagion, and conspiracy Ideation. Linguis Philos Invest 2020;19:128. doi:10.22381/LPI19202010OpenUrl↵Magarini FM, Pinelli M, Sinisi A, et al. Irrational beliefs about COVID-19: a scoping review. Int J Environ Res Public Health 2021;18:9839. doi:10.3390/ijerph18199839↵Vranic A, Hromatko I, Tonković M. "I did my own research": overconfidence, (Dis)Trust in science, and endorsement of conspiracy theories. Front Psychol 2022;13:931865. doi:10.3389/fpsyg.2022.931865↵Carrion-Alvarez D, Tijerina-Salina PX. Fake news in COVID-19: a perspective. Health Promot Perspect 2020;10:290–1. doi:10.34172/hpp.2020.44OpenUrl↵Kuhn TS. The structure of scientific revolutions. Chicago: University of Chicago Press, 1962.↵Callon M, Lascoumes P, Barthe Y. Agir Dans UN Monde incertain: Essai sur La Démocratie technique; 2001.↵Eysenbach G. How to fight an Infodemic: the four pillars of Infodemic management. J Med Internet Res 2020;22:e21820. doi:10.2196/21820↵Braun V, Clarke V. Thematic analysis: American psychological association. 2012.↵Wellcome T. Wellcome global monitor 2018: how does the world feel about science and health?; 2019.↵Bromme R, Mede NG, Thomm E, et al. An anchor in troubled times: trust in science before and within the COVID-19 pandemic. PLoS One 2022;17:e0262823. doi:10.1371/journal.pone.0262823↵Lee JJ. Party polarization and trust in science: what about democrats Socius 2021;7:237802312110101. doi:10.1177/23780231211010101OpenUrl↵Allea. Fact or fake? Tackling science disinformation. ALLEA Discussion Paper; 2021. 1–24.↵Chu L, Fung HH, Tse DCK, et al. Obtaining information from different sources matters during the COVID-19 pandemic. Gerontologist 2021;61:187–95. doi:10.1093/geront/gnaa222OpenUrl↵Constantinou M, Kagialis A, Karekla M. COVID-19 scientific facts vs. conspiracy theories: 0 – 1: science fails to convince even highly educated individuals. In Review [Preprint] 2020. doi:10.21203/rs.3.rs-33972/v1↵Winter T, Riordan BC, Scarf D, et al. Conspiracy beliefs and distrust of science predicts reluctance of vaccine uptake of politically right-wing citizens. Vaccine 2022;40:1896–903. doi:10.1016/j.vaccine.2022.01.039OpenUrl↵Bin Naeem S, Kamel Boulos MN. COVID-19 misinformation online and health literacy: a brief overview. Int J Environ Res Public Health 2021;18:8091. doi:10.3390/ijerph18158091↵Antiochou K. Science communication: challenges and dilemmas in the age of COVID-19. Hist Philos Life Sci 2021;43:87. doi:10.1007/s40656-021-00444-0↵Hubble E. The nature of science, and other lectures. Huntington Library, 1954.↵Gawande A. The mistrust of science, the New Yorker 2016. Retrieved; 2021.↵Feinstein N. Salvaging science literacy. Sci Ed 2011;95:168–85. doi:10.1002/sce.20414OpenUrl↵Hendriks F, Kienhues D, Bromme R. Trust in science and the science of trust. Trust and communication in a digitized world: models and concepts of trust research; 2016. 143–59.↵Higgins K. Post-truth: a guide for the perplexed. Nature 2016;540:9. doi:10.1038/540009a↵Proctor RN, Schiebinger L. Agnotology: the making and unmaking of ignorance. California: Stanford University Press Stanford, 2008.↵Center for Countering Digital Hate. The Disinformation dozen 2021; 2021.↵Harambam J. Contemporary conspiracy culture: truth and knowledge in an era of epistemic instability. Routledge, 2020.↵Morin E. Rumor in Orleans. New York: Pantheon, 1971.↵Christensen M, Anson A. The great reset and the cultural boundaries of conspiracy theory. Int J Commun 2023;17:19.OpenUrl↵Lederer S, Davis AB. Subjected to science: human experimentation in America before the second World War. History: Reviews of New Books 1995;24:13. doi:10.1080/03612759.1995.9949143OpenUrl↵Frachon I. Médiator 150 mg: Combien de morts?: Éditions dialogues; 2010. 2010.↵Reverby SM. Examining tuskegee: The infamous syphilis study and its legacy. Univ of North Carolina Press, 2009.↵Heyerdahl LW, Vray M, Lana B, et al. Conditionality of COVID-19 vaccine acceptance in European countries. Vaccine 2022;40:1191–7. doi:10.1016/j.vaccine.2022.01.054OpenUrl
|







![[2404.01669] How COVID-19 has Impacted the Anti-Vaccine Discourse: A Large-Scale Twitter Study Spanning Pre-COVID and Post-COVID Era | Actualités "Fake News and Vaccinations" | Scoop.it](https://img.scoop.it/R3Nf-aV-zFCPDr3s1jV_-zl72eJkfbmt4t8yenImKBVvK0kTmF0xjctABnaLJIm9)