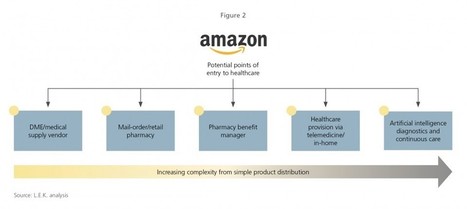
Amazon has been making waves in different parts of the healthcare industry over the past 12 to 24 months, but its recently announced alliance with JPMorgan Chase and Berkshire Hathaway demonstrated that Amazon’s ambitions go much further than simply selling healthcare products.
True, the initiative is still in its infancy and is limited to employees of the three partners, but the statement sparked a flurry of speculation and sent the stocks of insurers and major healthcare companies into a tailspin. Now that Dr. Atul Gawande has been appointed to lead this joint healthcare venture, many industry watchers are now asking: How far will Amazon, the master disrupter, take this?
Objectif : cet article vise la présentation et l’analyse des résultats statistiques d’une étude de corpus de communications vaccinales sur l’Internet. Dans une dynamique d’optimisation des discours sur le vaccin anti-papillomavirus humain (anti-HPV), nous chercherons à mettre en lumière les usages discursifs mobilisant surtout l’émotion, chez les acteurs médiatiques qui alimentent les controverses techno-scientifiques. Méthodologie : cette étude s’adosse à une approche segmentant les discours en diverses modalités « socio-communicationnelles », agissant dans le sens d’une mise en confiance, défiance ou encore hésitation vaccinale. Résultats : bien que de plus en plus de communications de santé préventive par vaccination soient symétriques vis-à-vis de leurs usages de modalités discursives mobilisant raison et/ou émotion chez leurs récepteurs, sur un Internet homogénéisant alors les représentations médiatiques pour le plus grand nombre, les présents résultats prouvent qu’il est néanmoins possible de mieux les caractériser pour mieux agir dessus, selon un équipement méthodologique nouveau (i.e. « l’approche socio-communicationnelle ») en permettant leur analyse fonctionnelle.
Authorship is the coin of scholarship — and some researchers are minting a lot. We searched Scopus for authors who had published more than 72 papers (the equivalent of one paper every 5 days) in any one calendar year between 2000 and 2016, a figure that many would consider implausibly prolific1. We found more than 9,000 individuals, and made every effort to count only ‘full papers’ — articles, conference papers, substantive comments and reviews — not editorials, letters to the editor and the like. We hoped that this could be a useful exercise in understanding what scientific authorship means.
Nutella, si cercano 90 assaggiatori. Ferrero offre il lavoro più bello del mondo per 2 giorni a settimana. Nessuna operazione di marketing.
Il lavoro più bello: Ferrero cerca assaggiatori di Nutella/ Nessuna operazione di marketing...
Nutella, si cercano 90 assaggiatori. Ferrero offre il lavoro più bello del mondo nella sede di Alba per due giorni a settimana e l'azienda assicura che non è un'operazione di marketing.27 LUGLIO 2018 - AGG. 27 LUGLIO 2018, 9.10 DAVIDE GIANCRISTOFARO ALBERTI
Nutella Ferrero cerca 90 assaggiatori - Pixabay
Sembra un sogno, ma è tutto vero: gli amanti della crema alla nocciola più famosa al mondo potrebbero realizzare il loro desiderio trasformando una passione in lavoro. La Ferrero, infatti, sta cercando assaggiatori per il suo prodotto più importante, la Nutella. Finora, tale compito era affidato al personale interno. L’azienda, però, ha deciso di allargare il giro assumendo delle persone esterne a cui verrà offerto un corso di formazione prima dell’inizio del lavoro durante il quale i futuri assaggiatori saranno educati al senso dell'olfatto e del gusto e a migliorare la capacità di esprimere a parole c’è che si percepisce con il palato. C’è chi vede dietro tale ricerca un’operazione di marketing, ma l’azienda assicura che la volontà è quella di garantire la qualità del prodotto e delle materie prime affidandosi al palato di quelli che sono i consumatori abituali della Nutella. Un lavoro golosissimo, dunque, che non vi ruberà molto tempo se non due giorni a settimana e che, quasi sicuramente, potrebbe rendervi le persone più felici di svolgere il proprio lavoro (aggiornamento di Stella Dibenedetto).
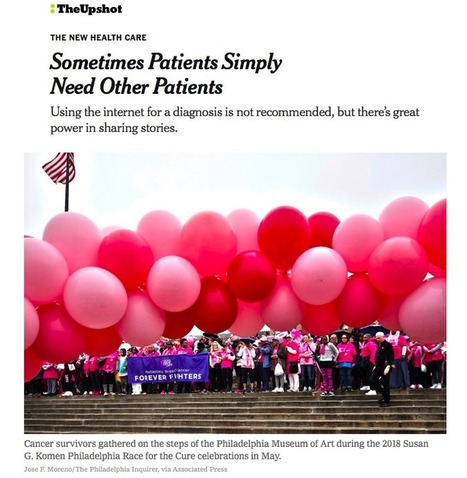
In an ideal world, when we are faced with a new health problem, a clinician is available to sit down and address all our questions and anxieties about the condition and its treatment. This ideal is rarely met in the United States health system. More typically, we’re rushed through doctor visits that fly by too quickly for us to gather our thoughts.
Other patients can help. They have (or have had) your condition, as well as your anxieties and questions, and they’ve found a path through. Their journeys can be informative and helpful, and can also help you prepare for the next session with a doctor.
This guide will walk you through how you can make smart food choices to reduce sugar consumption, and how you can keep your life sweet, even without so many sweets.
The randomized controlled trial is commonly used by both epidemiologists and economists to test the effectiveness of public health interventions. Yet we have noticed differences in practice between the two disciplines. In this article, we propose that there are some underlying differences between the disciplines in the way trials are used, how they are conducted and how results from trials are reported and disseminated. We hypothesize that evidence-based public health could be strengthened by understanding these differences, harvesting best-practice across the disciplines and breaking down communication barriers between economists and epidemiologists who conduct trials of public health interventions.
Four years ago, Toronto plastic surgeon Dr. Jamil Ahmad joined the social media platform Instagram to share pictures of a trip to the Middle East. More than 10 000 followers later, the account has become a powerful professional tool. He regularly posts before-and-after photos of patients, alongside family snapshots and gym selfies.
Ahmad said patients are “dramatically more informed” about surgery because of accounts like his. Many plastic surgeons and dermatologists have amassed large social media followings in recent years. South of the border, cosmetic dermatologist Dr. Simon Ourian has more than two million followers on Instagram, rivaling some of his celebrity clients, while plastic surgeon Dr. Sheila Nazarian has experimented with live-streaming procedures.
But as more doctors are showcasing their work on social media, others are questioning the ethics of posting about patients in such a public and informal space. At minimum, the rules for publishing patients’ information in journals, textbooks and educational presentations should also apply to social media, said Dr. Alireza Jalali, head of anatomy at the University of Ottawa’s Department of Innovation in Medical Education. “There are clear guidelines that people need to follow, and that’s, unfortunately, sometimes not done very well.”
Torna l’appuntamento con la cultura medico-scientifica: l’occasione per incontrare Premi Nobel, scoprire da vicino i progressi della medicina e confrontarsi con i temi di attualità. A Bologna dal 3 al 6 maggio la quarta edizione del Festival della Scienza Medica
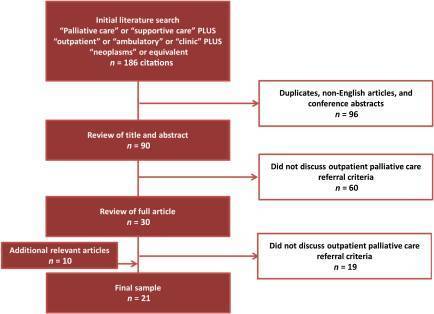
Outpatient palliative care clinics facilitate early referral and are associated with improved outcomes in cancer patients. However, appropriate candidates for outpatient palliative care referral and optimal timing remain unclear. We conducted a systematic review of the literature to identify criteria that are considered when an outpatient palliative cancer care referral is initiated.
Methods.
We searched Ovid MEDLINE (1948–2013 citations) and Ovid Embase (1947–2015 citations) for articles related to outpatient palliative cancer care. Two researchers independently reviewed each citation for inclusion and extracted the referral criteria. The interrater agreement was high (κ = 0.96).
Results.
Of the 186 publications in our initial search, 21 were included in the final sample. We identified 20 unique referral criteria. Among these, 6 were recurrent themes, which included physical symptoms (n = 13 [62%]), cancer trajectory (n = 13 [62%]), prognosis (n = 7 [33%]), performance status (n = 7 [33%]), psychosocial distress (n = 6 [29%]), and end-of-life care planning (n = 5 [24%]). We found significant variations among the articles regarding the definition of advanced cancer and the assessment tools for symptom/distress screening. The Edmonton Symptom Assessment Scale (n = 7 [33%]) and the distress thermometer (n = 2 [10%]) were used most often. Furthermore, there was a lack of consensus in the cutoffs in symptom assessment tools and timing for outpatient palliative care referral.
Conclusion.
This systematic review identified 20 criteria including 6 recurrent themes for outpatient cancer palliative care referral. It highlights the significant heterogeneity regarding the timing and process for referral and the need for further research to develop standardized referral criteria.
Implications for Practice:
Outpatient palliative care clinics improve patient outcomes; however, it remains unclear who is appropriate for referral and what is the optimal timing. A better understanding of the referral criteria would help (a) referring clinicians to identify appropriate patients for palliative care interventions, (b) administrators to assess their programs with set benchmarks for quality improvement, (c) researchers to standardize inclusion criteria, and (d) policymakers to develop clinical care pathways and allocate appropriate resources. This systematic review identified 20 criteria including 6 recurrent themes for outpatient palliative cancer care referral. It represents the first step toward developing standardized referral criteria.
Along with artificial intelligence, patient engagement feels like the new black in health care right now. Perhaps that’s because we’re just two weeks out from the annual HIMSS Conference which will convene thousands of health IT wonks, users and developers (I am the former), but I’ve received several reports this week speaking to health engagement and technology that are worth some trend-weaving.
As my colleague-friends Gregg Masters of Health Innovation Media (@2healthguru) and John Moore of Chilmark Research (@john_chilmark) challenged me on Twitter earlier this week: are we scaling sustained, real patient engagement and empowerment yet?
Let’s dive into the reports’ findings to divine an answer for Gregg and John.
Change Healthcare published the company’s 8th Annual Industry Pulse Report, which examines key challenges facing payors and other stakeholders this year. The report analyzes results of a survey of over 2,000 Change Healthcare customers (from academia, government, technology vendors, hospitals, providers, and health plans), conducted in October-November 2017.
Several findings address patient and health engagement in this study, including:
The failure of high-deductibles’ “skin-in-the-game” theory to turn patients into active health consumers
The growth of health plans and providers integrating social determinants of health into health strategies and tactics for improving peoples’ health outcomes and engagement
The migration of incentives from negative “sticks” to positive “carrots” along with more value-based benefit design in motivating consumer health behavior.
One of my favorite series of papers that inform my advisory work comes from PwC on the New Health Economy, this week publishing its report on Customer experience in the New Health Economy – the data cure. A highlight of their survey found that one-half of provider executives sees customer (patient, clinician) experience as a top strategic priority over the next 5 years, and most payer execs are investing in technology to improve member experience. Remember that health insurers rank very low on consumer experience compared with retailers and grocers.
PwC offers five pillars for healthcare stakeholders to build on to improve experience, including:
Convenience
Quality
Support
Personalization, and
Communication.
Finally, CarePayment studied the skin-in-the-game motivation for engagement, finding that 61% of patients don’t have money saved for healthcare expenses, and two-thirds of people have avoided or delayed medical care in the last year due to expected costs.
An alarming anti-engagement statistic is that 44% of the 1,000 consumers surveyed said they would not get needed medical care, even if it put their health at-risk, knowing they would have out-of-pocket expenses of $500.
The 20/20 CarePayment survey team also noted in their press release that among people who did not seek healthcare, medical debt is a growing and common problem impacting + nearly 1 in 4 Americans under 65.
The CarePayment poll was conducted in November-December 2017.
Health Populi’s Hot Points: So, Gregg and John, to your question: has patient empowerment and engagement scaled yet in U.S. healthcare?
Well, it depends on how we define the terms, and through what and whose lens. I do see green shoots of engagement among patients in the U.S., both for clinical activation and financial/shopping muscles.
A question in the Change Healthcare survey hints at one of the challenges in assessing and inspiring patient engagement: “What is the best approach for turning passive patients into active healthcare consumers?”
For many years, my discussions with patient activists on social media have informed me about some of the toxic language that prevents trusted conversations between people – patients, consumers, caregivers — and health care providers, plans, and pharma. Words like “adherence,” “compliance,” and in this question the verb, “turning,” are turn-offs for the very people legacy healthcare organizations want to engage.
Contemporary health engagement for patients in the U.S. is also complicated by the fact that patients are responsible for financing at least part of their healthcare — resulting in self-rationing among a large percentage of people who truly need to access care, the CarePayment survey points out. We’ve seen these behaviors based on other data sources, notably over the years via the Kaiser Family Foundation which I perennially cover — even back in 2012 before the advent of the Affordable Care Act.
As providers, payors and pharma allocate capital resources for technology to improve relationships with patients on the hardware side of the ledger, these healthcare organizations should also be mindful of other processes and mindsets facing consumer-patients — both in terms of helping people navigate the healthcare system, and at the same time, avoid the financial toxicity that can prevent them from seeking care in the first place.
Secondo il pensatore tedesco Hans Jonas l’uomo si realizza in un sano pensiero filosofico, evitando gnosticismo e storture scientiste Per non diventare delle «formiche tecnologiche»
«Che l’immagine dell’uomo non vacilli, si offuschi e sbiadisca, che gli uomini non si riducano a formiche tecnologiche o edonisti senza anima o marionette frastornate dal nostro furibondo potere». A cosa attingere per evitare questa deriva? All’uso adeguato della filosofia che instrada verso la vita buona e all’esercizio della virtù? Sono dilemmi che hanno il sapore dell’attualità benché sollevate da Hans Jonas nel 1955. Potrebbe d’altro canto essere diversamente se «le questioni filosofiche - puntualizzava il pensatore sei anni prima - si ripropongono ad ogni nuova epoca tanto daccapo, quanto alla luce della loro intera vicenda storica antecedente?». Le citazioni provengono dalle annotazioni del filosofo appartenenti alla sua stagione canadese, dal 1949 al ’55.
A lungo conservate all’Hans Jonas Nachlass dell’università di Konstanz sono state ripescate e raccolte in anteprima mondiale da Fabio Fossa in questo libro (Sulle cause e gli usi della filosofia e altri scritti inediti, Ets, pp.120, euro 10). Hans Jonas non è tra gli autori più conosciuti al grande pubblico eppure il suo curriculum scintilla. Dopo gli studi con Rudolf Bultmann e Martin Heidegger nella Germania degli anni Trenta, prende la via dell’esilio, lontano dall’Europa. La sua vita però non si riduce a studio e contemplazione. Anzi l’agire ne costituisce una cifra di rilievo. Lo prova, nel corso della Seconda guerra mondiale, la scelta di arruolarsi nella Jewish Brigade, inquadrata nell’esercito britannico e operativa sul suolo italiano. I rapporti con la penisola scandiscono la vita di Jonas. Sarà proprio al rientro dall’Italia, nel 1993, dopo avere ricevuto il Premio Nonino dedicato ai maestri del nostro tempo, che il filosofo tedesco naturalizzato americano si spegnerà a New York all’età di novant’anni.
The Delaware Division of Public Health (DPH), the University of Delaware’s School of Public Policy & Administration, and other partners created the Health Equity Guide for Public Health Practitioners and Partners to help Delawareans better understand tools and strategies that promote health equity and support upstream population health approaches. The 179-page document is designed to assist all sectors which can include but are not limited to government, education, workplaces, private sector, nonprofit agencies, faith based institutions, and health care settings address underlying causes of health inequities in communities and promote optimal health for all in Delaware.
Background
Our overall health is strongly influenced by where we live, learn, work, play and pray. It is also heavily influenced by your income level, education, and health care services. Our culture, language, political and religious beliefs, social norms and attitudes, and the rates of poverty, crime, and violence also affect our health. Delaware can achieve greater health equity as its environmental, social, and economic conditions improve.
The Division of Public Health (DPH) is working with many community leaders, non-profit organizations, other state agencies, and stakeholders to address health equity issues within our state and improve overall health for Delawareans. By engaging in healthy behaviors and improving environmental and social conditions, there is less risk of disease, disability, and injury. In order for this to occur, we all need to ensure that the healthy choice is not just the easy choice, but that it is also a possible choice within communities. The guide show cases existing evidence-based practices, tools and resources that can assist Delawareans to reach their full health potential and improve their overall quality of life.
DPH contracted with the University Of Delaware (UD) to develop the guide with the purpose of increasing awareness of DPH staff and other partners across the state and bring us closer together to address health equity issues in Delaware. This guide explores the major themes, frameworks, and approaches regarding health equity, all while keeping the context of Delaware in mind. The Health Equity Guide for Public Health Practitioners and Partners shares evidence-based and promising strategies, and provides numerous references and web links for additional information.
We proudly present the final product and can provide technical assistance and support.
Using the Guide
Everyone, no matter what sector you work within, can utilize the guide to prioritize health equity in their overall work.
Health inequities are historically entrenched and pervasive, but they are not insurmountable. We can be most effective by transforming our collective thinking from a perspective focused on treatment of the individual, to one that focuses on prevention, health, and wellness of the broader population. The guide provides a call to action for all of us to make fundamental shifts in our approaches.
The Guide was developed to be adaptable to all types of audiences – from academicians to grass roots community groups – and includes digestible strategies which highlight Delaware specific and national examples. The Guide is best utilized as an electronic file due to the inclusion of hyperlinks.
September 24, 2018 - This is the second of a three-part series centered on the steps required to make a patient engagement initiative successful. The first article, Three Steps to Jumpstart Effective Patient Engagement Initiatives, focused on jumpstarting an initiative. The final article will focus on the positive outcomes for which you can aim.
Once a comprehensive patient engagement initiative is agreed upon, the next step is to focus on an effective implementation plan.
Many tech-based implementation phases have an explicit beginning and end. The project team executes a project plan, installs some new software, and — voilà — problem solved. But patient engagement initiatives require an ongoing commitment.
As noted in the first installment of this three-part series, an effective patient engagement strategy depends on fundamental changes in organizational behavior and continual process improvements. As an organization’s needs evolve, the solution must be optimized as new staff and patients come on board, technology changes, the regulatory environment evolves, and so forth.
A patient engagement strategy must align with the overall organizational/business strategy. An organization’s staff, their skills, and the messages that surround a patient engagement system will contribute to its success. Change must occur across an organization to achieve the desired engagement outcomes.
Launching a patient engagement program is a bit like adopting a pet. The owner reaps many benefits, but it changes daily life. A comprehensive patient engagement system requires a commitment to new ways of communicating on a day-to-day basis.
STEP 1: SETTING THE STAGE FOR SUCCESS
Like so many things in life, success will depend on the effort and planning invested. While one might think implementation is largely about an effective project plan, the success of an initiative actually depends on persuading the many people who will be affected by this initiative of its value. Without a belief in the organizational change to be implemented, the best project plan is going nowhere.
Build a cross-functional team: Some organizations opt to create a new position to manage this initiative, which is not really necessary. In fact, since the organization is implementing a strategy that will affect the entire system (which may involve hospitals, clinics, individual medical practices, and so forth), it’s more effective to build a team that includes front-line staff and leaders who have experience in working with and navigating the organization.
Appoint a champion: This individual must have strong experience in leading, managing, and motivating teams. The champion should be passionate about the concepts, skilled at articulating the mission, and good at connecting with people. This person must sell this initiative team by team and get each one fired up about a new way of working. The reality is all of an organization’s competitors are doing the same.
Assign a project planning or operations professional: Consider teaming the champion with a project management specialist. This individual can keep everyone on track once the project plans are developed.
Internal and external communications: Selling a new vision for patient engagement requires a marketing and communications campaign to an array of constituents. A list of three-to-five key messages will form the foundation for all initial outreach. They must underscore not just the how, but the why, of the approach. Stress the benefits to patients and to staffers.
Executive announcement: Consider launching with an announcement from a top executive, setting the tone that this represents an organization-wide change. Depending on the size of the organization, this might require an all-hands meeting, a video, or an email, so that everyone gets the same message.
Keep communicating: Keeping everyone up-to-date takes time, but it is critical to success. This requires that everyone affected, including patients, be informed of pending changes. It also involves setting expectations, so that staffers and patients can anticipate next steps.
STEP 2: PROJECT PLANNING AND IMPLEMENTATION
Patient engagement implementation works best with a decentralized approach. While the overall strategy is likely centralized, outcomes and objectives in each subgroup or practice area are different. Allow flexibility for each department, floor, clinic, or hospital to define its own successes. This improves implementation outcomes and promotes participation. It’s simply more interesting to work on an initiative that you feel meets your daily needs.
Segment the organization into logical sub-groups: For each sub-group, establish a cross-functional team of stakeholders. Build a group with a positive, can-do attitude. Camaraderie is key.
Meet with each team: Offer five to ten measurable goals or outcomes the team can accomplish with the new patient engagement technologies. Let team members brainstorm to address the business problems they want to solve for their clinic, hospital, or practice. Ask the team to prioritize their objectives and discuss how the organization’s new tools can address them.
Develop sub-group-specific project plans: The business problems of a hospital will differ from those of a clinic. Their plans will therefore vary, but some elements will be consistent. While this may initially add complexity to the implementation, tailored project plans will yield a sense of ownership on the part of the teams. As a result, they will help sell the vision internally, which will result in higher utilizations.
Test concepts with patients: After all, patient activation and participation are central to your patient engagement strategy. Don’t assume that you know how patients will respond to various outreach and engagement strategies. What works for a patient with a high degree of health literacy may not work for a healthy young person who has had little exposure to the healthcare system. Some organizations feel it’s a mistake to have patients meet directly with the project teams, preferring to gather input via focus groups and summarizing it for the team. But the staff will benefit by hearing from patients directly. In turn, patients will be more engaged in the process, offering more candid, valuable feedback.
Deal with doubters: When implementation begins, the naysayers will speak up. Be prepared with facts and creativity. For example, at one organization a physician was a bit skeptical about engaging patients via technology, but she wanted to help educate her diabetic patients with out-of-range A1C levels (i.e., a measure of blood sugar levels). As part of a project to recertify for her internal medical boards, she instructed her patients to watch a video about managing their diabetes on their phones before leaving the hospital parking lot. While it was a small sample size, her project revealed that 98 percent of patients watched the video as instructed. Within six months, 86 percent of those patients had in-range A1C values.
Leverage vendor experts: While some aspects of a project plan will be unique to the organization, it’s safe to assume that the vendor has seen many of the issues you encounter during implementations time and again. The vendor should be a business partner who can help accomplish your business goals. Let the vendor team guide the implementation process and the initial steps of staff training. Take full advantage of the vendor’s experience. They’re invested in your success; a happy customer makes a happy reference.
The testing phase: As part of the project plan, the team will need to consider the testing phase. Will you go live in an entire community or sub-group? A subset of that group? How will you measure success for each group? Be prepared for the worst. Invariably, the problems that you’ve worried about most will go flawlessly. Other issues will jump out instead.
For example, in one implementation, the team underestimated patients’ concerns about the possibility of a phone or email scam. After a patient received an automated follow-up call from the new system, he contacted the health system’s legal team to report it. The implementation team had failed to keep the legal staff in the communications loop, which led to some uncomfortable phone calls. This situation is a reminder that communications strategies need to include everyone in the organization, and that patients need to be alerted to the types of communications they’re going to receive.
STEP 3: OPTIMIZING UTILIZATION
Once the teams have completed the initial rollout of their new patient engagement solutions, everyone breathes a collective sigh of relief. But the work has just begun. The organization has embarked on a new path. It will take time to fine-tune processes and to get the whole organization rowing in the same direction.
Recruit the vendor to help with utilization optimization: How can processes and tactics be fine-tuned to make sure the organization is getting maximum value out of the product?
Reinforce the long-term gains: Continually report to executive leadership, staffers, and patients on the benefits of using technology to engage. Actual stories from patients combined with solid outcome data is the best. Share successes internally and externally.
Handling staff turnover: The process of staff engagement and education is ongoing. As staffers change roles or leave the organization, how will staff education be managed beyond the initial implementation phase?
Engaging new patients: As new people come in the door of your hospital, clinic, or office, what is the plan for getting their attention? A recent survey indicated that individuals who were encouraged by their clinician to use online medical records were nearly two times more likely to access their record compared to those who were not encouraged. One practice found it effective to have a staffer take five minutes with new patients on their first visit to get them signed into their portal. It removed one communication barrier for many patients.
Reach out to existing patients: If patients aren’t using the portal or watching videos, can someone on the staff call or email to find out why? A staffer might ask, “I see that you got a call from an automated system with these questions, but you didn’t respond. Would you find an email more effective?”
Appeal to different patients and their circle of care: Patients’ needs are different. Some require expectation management while others require solid coaching and encouragement. The needs of a 30-something primary care patient who gets a physical once per year are different than those of a patient with a chronic condition. Family members caring for an elderly parent have different needs than existing patients facing surgery for the first time, whose questions and concerns may be driven by fear. Over time, patient engagement strategies must be tailored and expanded to better serve the various patient constituencies.
An ongoing commitment to success: To keep patients and staff engaged, the organization must continually iterate, adapt to changing technologies, solicit feedback, and employ creativity.
About the Author: Pam Holt, RN, BSN, MOL, is operational consultant for patient engagement with Clinical Effectiveness at Wolters Kluwer, Health. In her role, Pam helps deliver measurable business outcomes through patient engagement strategies. Prior to joining Wolters Kluwer, Pam served as the System Director for Patient Education at Mercy Health System, based in Chesterfield, Missouri.
About the Sponsor: Wolters Kluwer Health is a leading global provider of trusted clinical technology and evidence-based solutions that engage clinicians, patients, researchers, students and the next generation of healthcare providers. With a focus on clinical effectiveness, our proven solutions drive effective decision-making to reduce variability and produce consistent outcomes across the continuum of care. Healthcare professionals around the world use our trusted solutions, such as UpToDate®, Lexicomp®, Medi-Span®, and Emmi® patient engagement programs.
"Somewhere along the way, doctors became “providers.”
And while some physicians have raised objections, the term provider is still being used—and it still doesn’t work, says Jennifer Weiss, M.D., an orthopedic surgeon, in a post on KevinMD.
“Calling medical doctors 'providers' does more than inflict eco-injury. It actually reduces morale, worth, purpose and results in already overworked doctors finding less meaning in the work that they do,” says Weiss.
In the corporate world, the pendulum is swinging back to using job titles that actually define an employee’s role accurately. But the trend hasn’t found its way into the medical world, Weiss says. Instead, the word provider, a term that doesn’t reflect a person’s training or tasks, has come into fashion.
The term was adopted by federal law in the early 1970s and by its definition can include everyone from a doctor of medicine or osteopathy to a nurse practitioner or clinical social worker.
It’s not just doctors who should be bothered by the term, Weiss says, arguing there is nothing “mid-level” about a so-called mid-level provider who works long shifts and takes care of sick patients.
“The whole term (any way you put it) doesn’t work and needs to be changed,” she says. “...Why is anyone on a medical staff still being termed “provider” if we know that titles matter, are used to accurately reflect a person’s role within a company and lead to better overall engagement in the workplace? It’s not only nonsensical, but it’s also detrimental,” she says.
In fact, healthcare professionals have different training, knowledge and clinical experience. In the shift to team-based care, members have different roles and responsibilities based on their specific competencies."
This film records an in-depth interview with French artist Marcel Duchamp [1887-1968] which took place five years before his death, at the time of his first ever one-man show (at the Pasadena Art Museum). It records for posterity Duchamp talking about his life, his ideas on art, why he chose to continue living in America after fleeing France in 1915, and why he virtually abandoned his work as an artist in 1923. While he is most often associated with Dada and Surrealism, his participation in Surrealism was largely behind the scenes, and after being involved in New York Dada, he barely participated in Paris Dada. An engaging dialogue takes place between Duchamp and film-maker Jean-Marie Drot as they go around the Pasadena show, with the artist commenting on the exhibits and using them to explain the various stages of the development of his work. This is punctuated by the games of chess, which were for Duchamp a passion and a metaphor for the mental discipline he applied to his art. In this film we gain a rare glimpse of him talking with humour and insight about his ideas, and living up to the myth of the artist-philosopher that has grown up around him. Jeu d'échecs avec Marcel Duchamp was filmed late 1963 in Pasadena and New York for the Radio Télévision Française (RTF); first broadcast on 8 June 1964 and then shown at the International Festival of Artistic Films and Films of Art (Bergamo, 19 September 1964). A videocassette was issued by Public Media, Chicago 1987 (Marcel Duchamp. A Game of Chess) and by Phaidon (2007). The English version was presented in a television broadcast in September 1964 in the 'Art and Man' Series.
Che cosa significa «engagement»? Si tratta di un coinvolgimento attivo dei pazienti nel Sistema sanitario nazionale. Per arrivare a un modello partecipativo in sanità serve un cambiamento culturale. Ne parla nella video intervista Guendalina Graffigna, professore associato di Psicologia all’Università Cattolica di Milano.
Our health needs change with every passing decade, but the good news is that it's never too late to start taking better care of yourself. Whether you are in your 30s, 40s, 50s or beyond, the Well Midlife Tuneup will put you on a healthier path to improving your body, mind and relationships. You are only as old as you feel, and completing our tuneup will definitely help you feel young at heart. Let's get started.
Within the next three to five years, the use of social media to connect with individuals is expected to increase by 256%.
For the health care industry in particular, social media can help engage patients, providers and the public with relevant and timely information, as well as communicate the value and credibility of a health system.
Why is this tactic becoming a critical component of health care marketing strategy?
A recent study found 57% of consumers’ decisions to receive treatment at a health care facility are strongly influenced by that provider’s social media connections, showing that patients trust health organizations with a social presence.
According to another report, 60% of doctors say social media improves the quality of care delivered to patients, which means that doctors also value the transparency and open communication that social media can provide.
With the opportunity to increase patient referrals and improve the quality of care, it’s no surprise that many health systems are jumping on the social media bandwagon.
Let’s take a look at a few ways using social media in health care can improve overall marketing efforts:
Engage With Patients in Real Time
One of the benefit of social media marketing in health care is enabling deeper and more meaningful discussions that address patient questions, concerns and interests in real time.
The question is, how can health care marketers effectively use social media to communicate and engage with existing patients?
Health systems can facilitate patient empowerment by enabling and engaging in patient forums and research networks online. For example, PatientsLikeMeallows patients to manage their own health conditions by discussing treatments with patients who have similar conditions. Hospitals and other health networks can develop their own platforms that allow patients to share their experiences and receive support from similar individuals.
Along with forums, health systems can use social networking pages to encourage patient discussions. For example, Children’s Mercy uses their Facebook page to showcase their reputation as a renowned care center.
“Locally, Children’s Mercy wants parents to know their kids are in good hands. Social is a good way to share news and feature CMH doctors and patients,” says PR director Jake Jacobson.
This video is a part of Children’s Mercy’s “Big Slick KC” promotion for their annual fundraiser. Posts like these raise awareness for the health system’s Cancer Center, share patient stories and urge people to donate.
According to the Journal of Health Management, “When patients tell their stories, their friends see that, and the likelihood of spreading the message increases many-fold.”
To successfully engage patients on social media forums or networking sites, organizations must regularly monitor these platforms to respond to patients in a timely manner, as well as ensure fresh, engaging content is added often to keep patients interested.
Facilitate Physician Collaboration
Health care marketers can also use social media channels to encourage physician alignment and collaboration. Texas Health, a network of 25 hospitals that employs 5,500 physicians, created an enterprise social networkto help physicians communicate and work with one another to overcome challenges posed by the work environment, such as electronic health record requirements.
As a result of this networking initiative, the health system saw improved physician collaboration, a shorter learning period and greater acceptance of social media tools.
Social media is an easy way for physicians to find and connect with other health professionals, even those outside of their own health system or hospital. Physicians can also share their knowledge or research to benefit other providers.
Overall, these practices improve physicians’ knowledge and willingness to work as a team. The more informed and educated a health system’s physicians are, the happier patients will be with their experience and the quality of care provided.
Ultimately, health care marketers should strive to provide patients with better experiences to foster loyalty, retention and positive word-of-mouth referrals. Improving physician engagement and alignment is one way to do so.
Support Population and Preventative Health Initiatives
Since many social media sites are public communication platforms that can reach a wide breadth of individuals, health care organizations can use this marketing tactic to support broader population health and preventative health initiatives.
One way to do this is to communicate educational information about health events and crises. Lee Aase of Mayo Clinic and Shannon Dosemagen of Public Laboratory for Open Technology and Science, say “organizations can use social media to distribute time-sensitive health information, promote information sharing to encourage behavioral changes (including corrective changes during potential health crises), be a platform for conversation between agencies and constituents (rather than just as an information provider) and allow the public to provide useful information and feedback.”
Health care organizations can also use social media as a platform to distribute information about common health conditions, diseases and other public health issues as a preventative measure.
As John Weston, CMO of Mayo Clinic notes, “We leverage the rich content we have to provide consumers with information about diseases and conditions, even when it is likely they may never become a patient. We view this as part of our moral responsibility — to share our knowledge and expertise to benefit others.”
Though social media provides the opportunity for health care organizations to reach large consumer and patient populations, marketers need to be mindful of maintaining HIPAA compliance and other privacy regulations on these public platforms.
Providers can maintain the trust of patient-provider relationships by staying far away from patient information and establishing a professional presence. Keeping this in mind, social media in health care has the potential to improve patient engagement, drive physician alignment, and foster a healthier society overall.
How does your healthcare organization take advantage of social media?
Nous qualifions souvent les produits de santé comme «des produits du quotidien pas comme les autres ». Cela est dû à leur haut niveau de spécificité tant scientifique que technique, mais également à leur place privilégiée dans notre société hautement soucieuse de sa santé.
Over the last decade, the Center for Medicare and Medicaid Services (CMS) has created both mandatory and voluntary programs designed to move healthcare providers from fee-for-service payment models to those that are value-based. Some of the most well-known programs are bundled payments.
Bundled payments have proven challenging for providers to address, as oftentimes they are unsure where or how to start. The shift towards value-based programs like BPCI (voluntary bundled payment program) and CJR (mandatory bundled payment program) have become a dividing issue amongst healthcare executives as some doubt the programs will drive desired success. More often than not, forward-thinking and progressive providers are already positioning themselves for the future by putting into place the right processes and structures for success.
Overall, consumers cite three key things that could improve the doctor-patient relationship: greater connectivity, better convenience via text and online tools, and more time with the doctor.
Brands and marketers alike have many things to consider in today’s ever-changing healthcare landscape. Are patients happy with their relationships with their healthcare providers? How likely are they to switch doctors? What could be improved with the doctor-patient experience? How do people want to be communicated with by their providers’ offices?
Millennials Among the three generations, Millennials are the least satisfied with their doctors and are most likely to switch practices. Not surprisingly, the researchers found that they are also the generation that is most likely to want to receive e-mail and text communication from offices.
Generation X Many Generation Xers control healthcare decisions across multiple generations, and their preferences and satisfaction levels both fall somewhere between younger and older consumers. Overall, the researchers found that they are fairly similar to Millennials, with an openness to digital communication and to switching providers.
Baby Boomers Baby Boomers, the biggest consumers of healthcare services, are the least likely to switch doctors. However that doesn’t necessarily mean they’re happy: less than half are satisfied with their current providers. Boomers are also the generation least interested in receiving communications from doctors’ offices digitally.
"We don't want to miss the train of digital health" is a phrase Bertalan Mesko, MD, PhD, has heard many times since he started working with pharmaceutical companies. Well, I have good news, says Mesko. They cannot miss it, because there are no trains to catch anymore. Instead, we should be looking to futuristic spaceships. If the pharma industry doesn't deal with disruptive technologies, it won't have an industry at all.
It might sound like a bold statement, but major trends suggest a future in which medical innovations come from a garage or a small startup company. For hundreds of years, innovation belonged to the R&D departments of pharma companies. A few technological developments might change that forever – and we are not happy about it.Bertalan Mesko, MD, PhD
"Complex question indeed that you raise about the transformation of pharma. So far, pharma has mostly missed out on the opportunities to 1) communicate in an engaging way on social media 2) to be involved in mobile apps that are used in a significant way 3) to transform their relationship and the sales process toward healthcare professionals 4) to transform internal processes in general. So, that's a poor scorecard indeed.
"However, if we look at, for example, Silicon Valley start-up accomplishments in health, there have been hiccups as well.
--Companies without pharma/device experience such as 23&Me and now Theranos turned out to have made premature announcements, probably to satisfy investors, and then faced setbacks.
--Healthcare connected objects and apps, even when not suffering from restrictive pharma marketing policies, confront high abandonment rates and seem to have difficulties in demonstrating clinical value.
"For the moment, even monster Google seems to want to partner with pharma rather than go it alone, (although this can change once Google has learned how everyone works from the inside).
"Wouldn't it be fair to say that new, disruptive ideas have always started with individuals or tiny teams. Many pharma compounds were the work of external researchers that were licensed or brought in.
And pharma is now taking a close look at start-ups and finding ways to collaborate with them as they would have with academic researchers in the past."
A good example of pharma collaborated with start-ups is Bayer's Grants4Apps™ program, which invites health app developers to submit their innovative app ideas for novel software that contributes to improving health outcomes. For more on that, see: http://bit.ly/pgtourberlin2013
In meno di tre giorni si sono accumulati nel mio cellulare (uno di prima generazione) 418 messaggi. Anzi, messaggini, secondo il lessico lezioso e vezzoso che adorna di fiori di carta le gabbie d’acciaio della tecnologia. Telefonini, messaggini, ditini che battono tastini. Non so cosa dicano, quei 418 appelli in una bottiglia, perché non sono capace di leggerli e dunque di rispondervi. Non è una stolida posa antitecnologica, sempre falsa e patetica, non solo perché si disconosce con supponenza l’aiuto che la tecnologia reca alla vita — basta pensare alla medicina e alla chirurgia — ma anche perché si crede che la tecnologia sia solo quella recente, quella che è piombata nella nostra vita già adulta, e si identifica la cosiddetta natura con la tecnica che c’era già quando si è venuti al mondo. La radio, ad esempio, mi sembra più «naturale» della televisione, perché quando sono nato i suoi suoni erano già nell’aria, come gli altri rumori della realtà, mentre la televisione è entrata a casa mia quando finivo il liceo. Nessuna psicosi o civetteria antitecnologica dunque, da parte mia. Semplicemente soffro di disabilità digitale, che è un handicap ma non una colpa, e invoco rispetto per questa mia «diversa abilità» digitale, come si dice in politically correct, così come chiedo comprensione perché non sono più in grado di fare le belle escursioni in montagna di una volta.
Tuttavia, direbbe Musil, in ogni più c’è un meno e in ogni meno un più. Se ne fossi stato in grado, avrei letto quei 418 dispacci e avrei risposto ad ognuno, come faccio con ogni lettera cartacea, almeno una quindicina al giorno. Calcolando 2,30 minuti per ogni lettura di sms e risposta, probabili controrisposte e mie relative repliche, avrei impiegato, credo, circa sedici ore. Due giornate di lavoro pieno, e verosimilmente altrettante nei tre giorni successivi e via di seguito. Dove resta il tempo per il lavoro col quale — a parte i pensionati, i milionari, i carcerati, i malati o i disoccupati — ci si guadagna di che vivere, e per leggere, passeggiare, incontrare gli amici, fare all’amore? Ai tavoli di ristoranti e caffè si vedono persone che non parlano tanto fra loro quanto con invisibili interlocutori al telefono e non solo un paio di volte, come sarebbe naturale, ma per quasi tutto il tempo che scorre fra l’antipasto e il dessert. Quando i due — o i quattro o cinque — cominceranno a parlare fra loro?
The evidence is clear: It's time to terminate pay for performance, the catchall term for policies that purport to pay doctors and hospitals based on quality and cost measures.
To get content containing either thought or leadership enter:
To get content containing both thought and leadership enter:
To get content containing the expression thought leadership enter:
You can enter several keywords and you can refine them whenever you want. Our suggestion engine uses more signals but entering a few keywords here will rapidly give you great content to curate.



 Your new post is loading...
Your new post is loading...